
The Common Vein Copyright 2008
Definition
Acute calculous cholecystis is an inflammatory condition of the gallbladder caused by obstruction of the cystic duct, usually by a small gallstones.
Structural changes include an inflammed, and distended gallbladder with a hyperemic wall
There is no specific functional impairment per se as result of the disease, except that less concentrated bile reaches the duodenum.
The disease may be complicated by perforation and bile peritonitis, and sometimes by empyema.
Clinically the patient presents with RUQ, with malaise and usually a fever. A positive Murphy’s sign is almost pathognomonic.
The diagnosis is best made by combining the clinical presenattion of right upper quadrant pain, positive Murphy’s sign, history of cholelithiais, with ultrasound findings of a distended hyperemic gallbladder that contains stones, fluid or comples stranding in the gallbladder fossa and probe tender gallbladder. The stones when impacted in the cystic duct are rarely visualized.
When the diagnosis requires confirmation the most specific study is a HIDA scan. CTscan is helpful to evaluate for local perforation by its ability to evaluate the pericholecystic fat.
Treatment is usually elective surgery, but the patient is traeated medically in the acute phase with antibiotics and pain medication.
 Acute Cholecystitis Acute Cholecystitis
Red Hot Gallbladder |
| The artistic rendering shows an enlarged, inflamed, red, hyperemic gallbladder consistent with the diagnosis of acute cholecystitis.
24761b01.99.8s gallbladder inflammation red cholecystitis acalculous calculous hemorrhagic rubor hyperemia dolor calor Davidoff art Courtesy Ashley Davidoff MD copyright 2008 |
The development of stones varies according to the different stone types:
Pigment stones are associated with: hematologic disorders with ? RBC survival, such as sickle cell disease, spherocytosis, thalassemia
In women, use of oral contraceptives has been associated with liver and biliary dysfunction, namely cholelithiasis and cholecystitis.
Interestingly, independent of other factors, diabetes, hypercholesterolemia, increased alcohol intake, and high parity are not associted with an increased risk of developing acute cholecystitis.
 Small Pigmented Stones Lying Dependantly in the Gallbladder Small Pigmented Stones Lying Dependantly in the Gallbladder |
| The stones that are most likely to cause obstruction and subsequent cholecystitis are the small stones rather than the large stones because the cystic duct is only 1-3 mms in diameter and therefore large stones cannot even enter the cystic duct. The diagram shows three small mobile stones with a patent cystic duct and infundibulum.
11921.8b05b018.8s gallbladder cystic duct gallstones cholelithiasis Davidoff Art copyright 2008 |
The pain of biliary colid is distinguished from that of acute cholecystitis by its intermittent nature and relation to meals as well as the absence of fever.

Stone Impacted in the Neck Causing Obstruction |
|
This diagram shows a small stone impacted in the neck of the gallbladder and the gallbladder has become distended. This diagramatically represents an early stage of cholecystitis before any significant inflammation has occurred. 11921.8b05b019.8s gallbladder cystic duct gallstones cholelithiasis stone impacted in the cystic duct distended enlarged Davidoff Art copyright 2008 |

Inflammation of the Gallbladder Wall |
| The longer the stone remains impacted, the more swollen the gallbladder becomes and the pressure on the wall causes ischemia and inflammation. The diagram shows a reddened and slightly thickened wall.
11921.8b05b020.8s gallbladder cystic duct gallstones cholelithiasis stone impacted in the cystic duct distended enlarged hyperemic wall acute cholecytitis Davidoff Art copyright 2008 |

Stone Impacted in the Cystic Duct |
| The stone can also become impacted in the cystic duct and the result is the same. There will be swelling of the gallbladder ischemia and inflammation. This diagram shows a small stone (green) stuck in the cystic duct and secondary distension and inflammation of the gallbladder wall.
04766b05b04b.35k.8s gallbladder cystic duct stone impacted obstruction enlarged gallbladder acute calculous cholecystitis Davidoff art copyright 2008 |

Inflammation of the Gallbladder Wall |
| The longer the stone remains impacted, the more swollen the gallbladder becomes and the pressure on the wall causes ischemia and inflammation. The diagram shows a reddened and slightly thickened wall.
04766b05b04b.36k.8s gallbladder cystic duct stone impacted obstruction enlarged gallbladder acute calculous cholecystitis Davidoff art copyright 2008 |
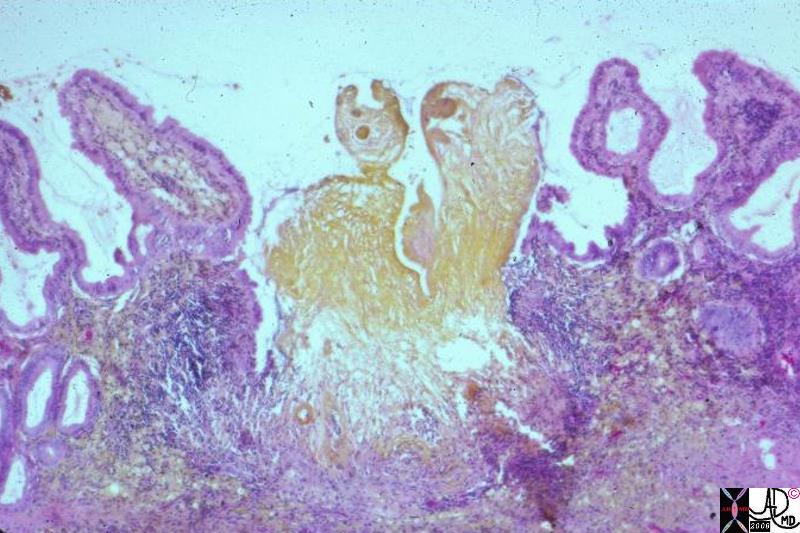
Applied Histology of the Gallbladder Fossa
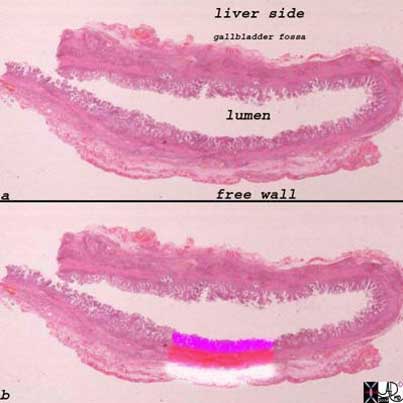
The upper and lower images represent whole mounts of a normal gallbladder. The upper image shows the liver surface of the gallbladder and the region of the gallbladder fossa, the lumen, and the free wall that is covered by the peritoneum.
The lower image shows the three basic histological layers. The pink mucosa, the red muscularis, and the white outer serosa.
Images courtesy of: Ashley Davidoff, M.D.2008
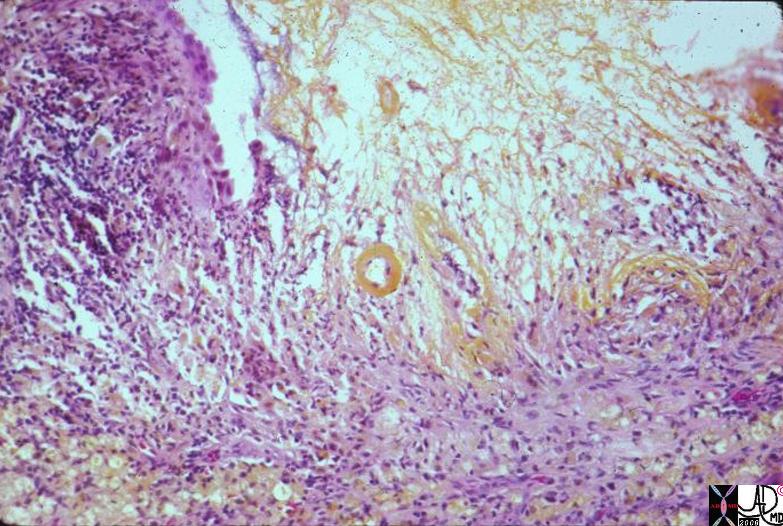
A closer look at the bare area of the Gallbladder
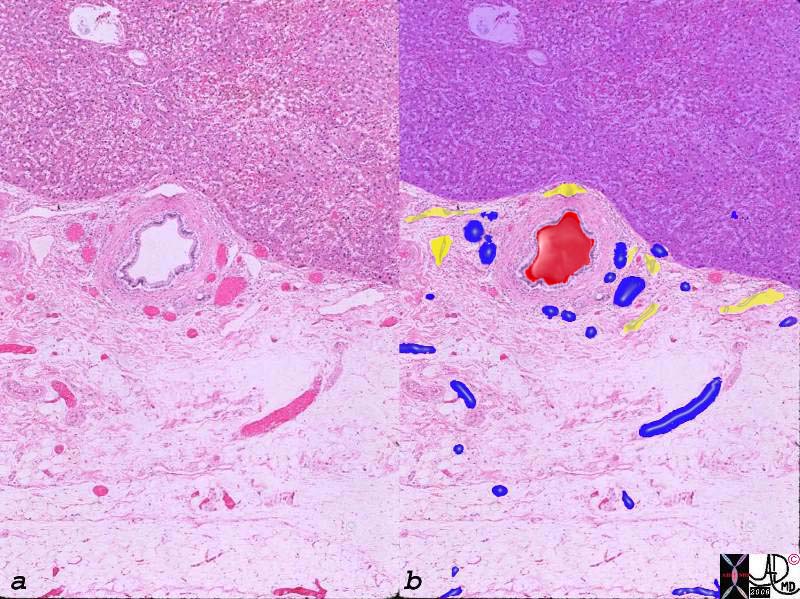
Arteries, Veins and Lymphatics in the Gallbladder Fossa |
|
The histological section of the gallbladder fossa shows the relatively large thick walled branch of the deep cystic artery, abutting the liver (upper portion purple) accompanied by venules (blue) and lymphatics (yellow). The veins and lymphatics drain directly into the liver. 00140c03.8s gallbladder wall gallbladder fossa normal artery duct liver interface histopathology |
The gallbladder fossa is rich in lymphatics
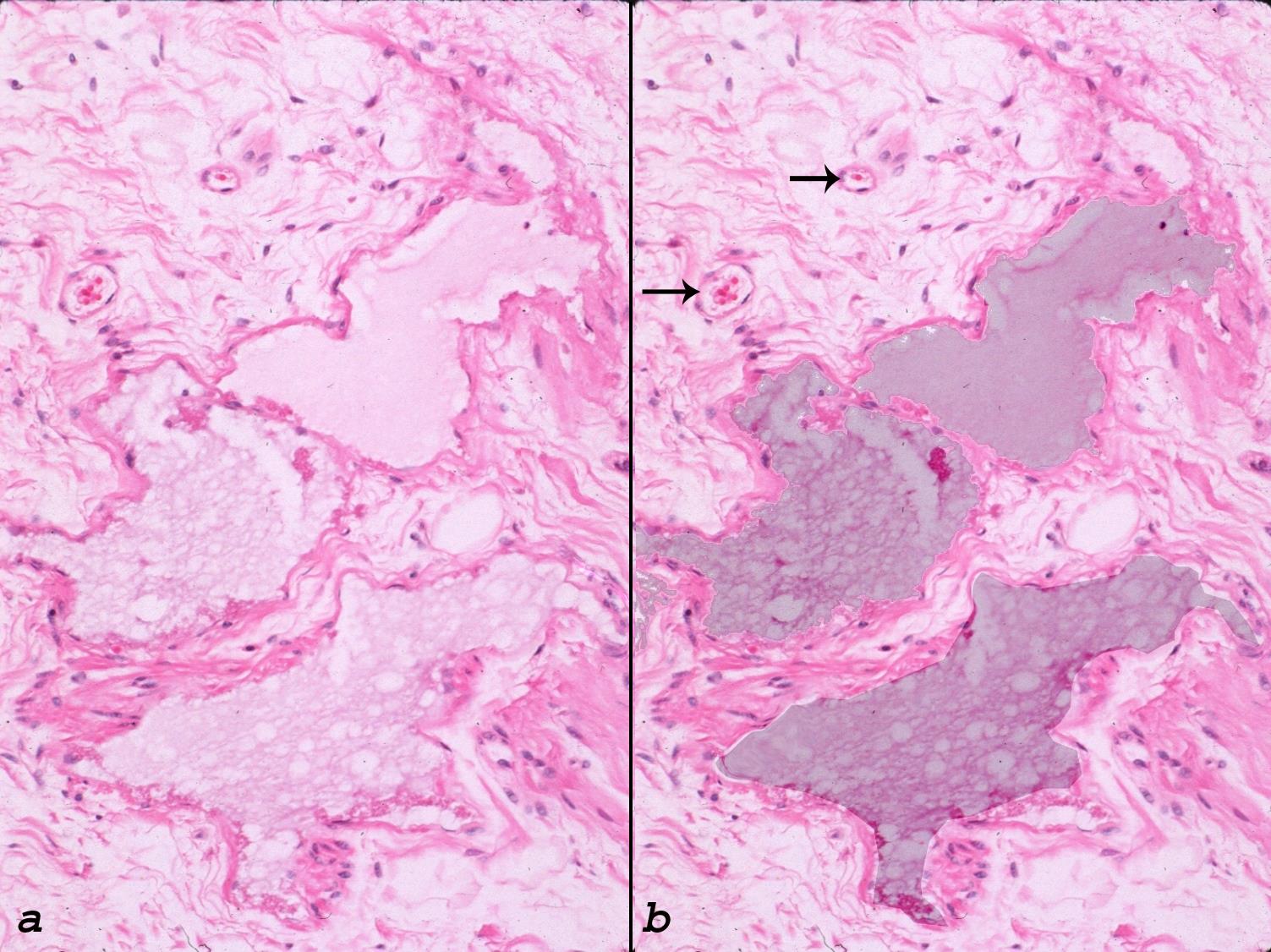
The gallbladder fossa is the hilum of the gallbladder and contains lymphatics, venules and arterioles and sometimes there is direct drainage of the biliary system into the gallbladder (duct of Luschka)
In acute cholecystitis there is hyperemia with increased blood flow, congested capillaries and increased leakage of fluids resulting in edema and increased lymphatic congestion , Since the histology of the bare area and free wall of the gallbladder are so different they have different imaging manifestations
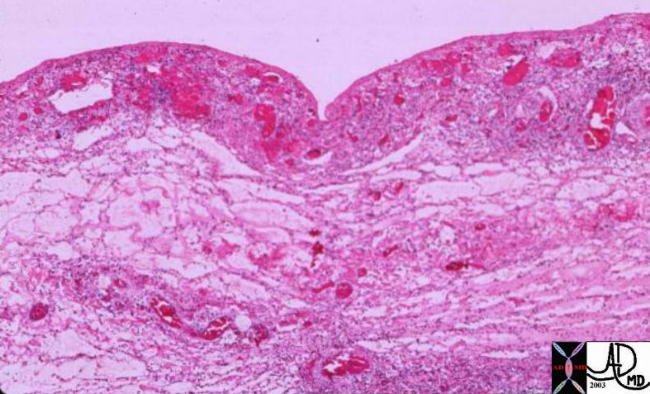
Hemorrhagic Congestion in the Gallbladder Wall |
| The histological section shows hyperemia, inflammation with a cellular inflammatory infiltrate as well as edema of the serosa and connetcive tissue.
00151 gallbladder wall inflammation acute cholecystitis histopathology |

Acute Cholecystitis |
|
The pathological specimen above shows a gallbladder with a thickened and hyperemic wall containing black pigmented metabolic stones. Histologically the findings were consistent with a diagnosis of acute cholecystitis. 02338 gallbladder + acute cholecystitis stones cholelithiasis + gross pathology |
As the inflammatory process progresses the veins and lymphatics become congested and since they are concentrated in the gallbladder fossa, fluid and fibrin start to accumulate in the fossa. The fluid may be seen as a hypoechoic region on US, while if fibrin predominates a lacy pattern is seen
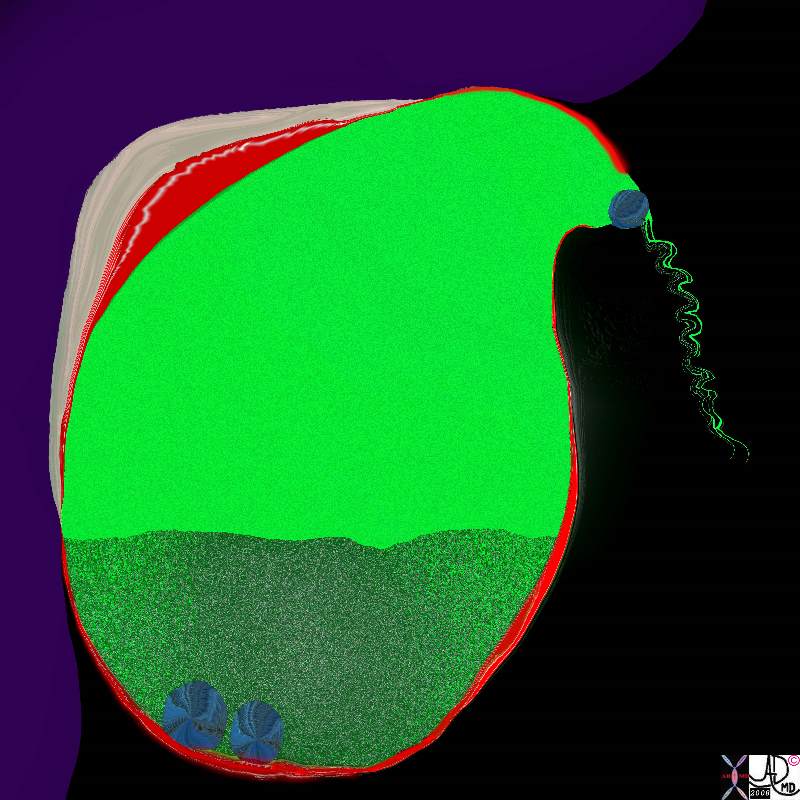
Complex Fluid in the Gallbladder Fossa |
|
As the inflammatory process progresses the veins and lymphatics become congested and since they are concentrated in the gallbladder fossa, fluid and fibrin start to accumulate in the fossa. The diagram above accumulation of fluid (beige) and red cells (red) in the gallbladder fossa. 11921.8b05b031.8s gallbladder cystic duct gallstones cholelithiasis stone impacted in the cystic duct distended enlarged hyperemic wall complex fluid in the gallbladder fossa tumefactive bile cholestasis sludge acute cholecystitis Davidoff Art copyright 2008 |
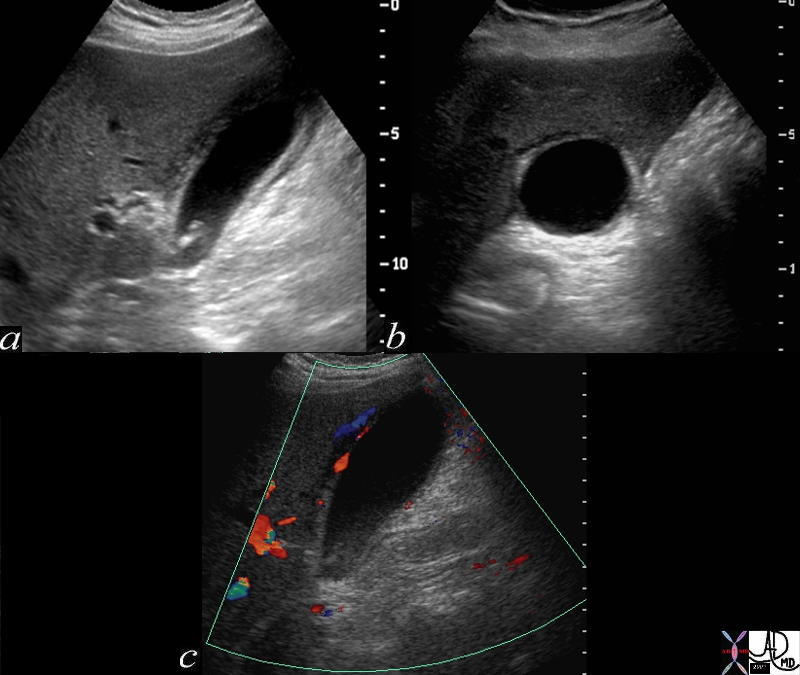
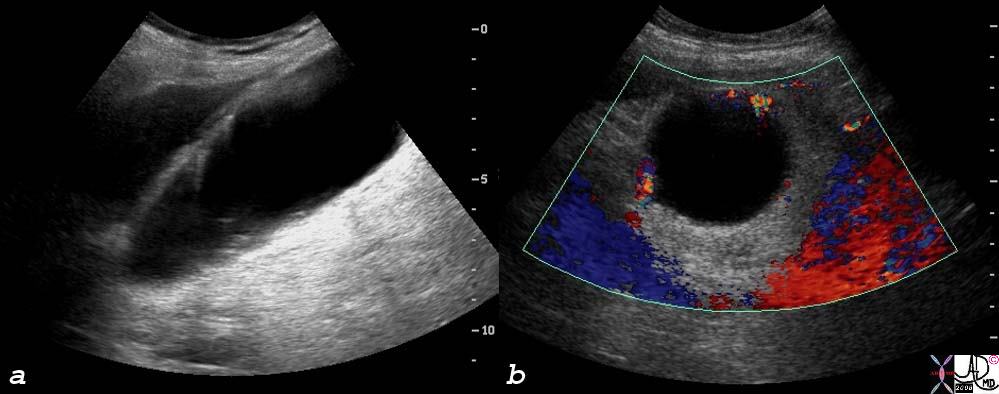
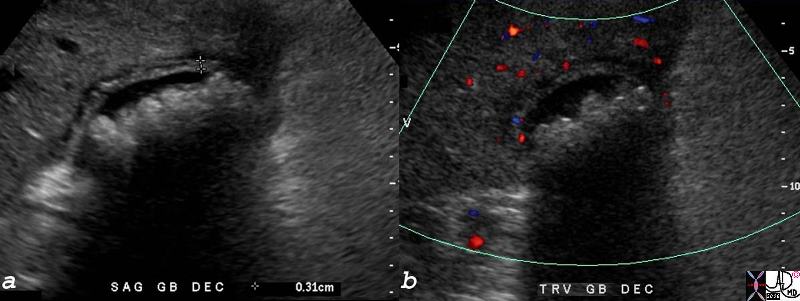
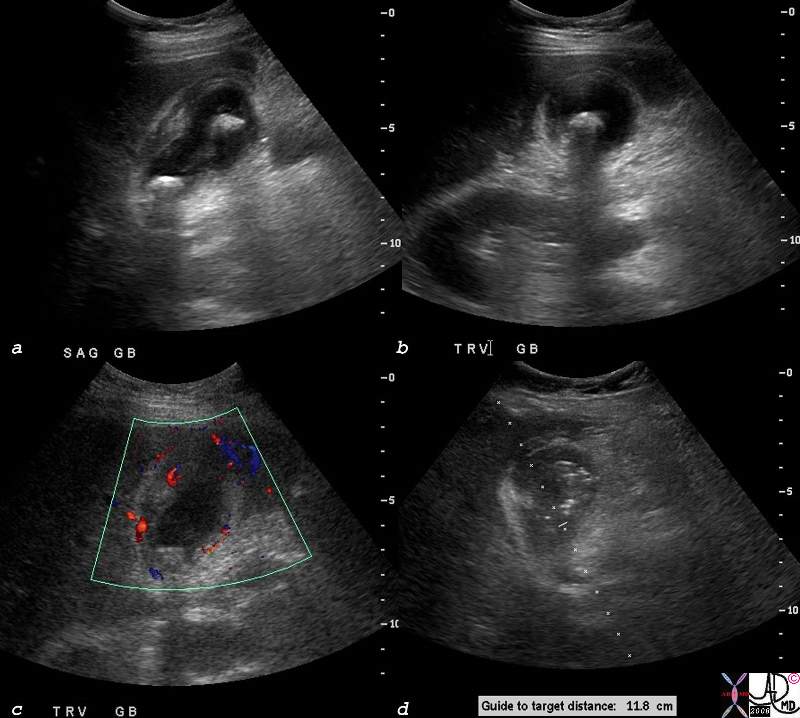
Acute Calculous Cholecystitis wit Gallbladder Wall Edema and Hyperemia |
| The three images depicted above are from a patient with acute cholecystitis. Image a shows the gallbladder in longitudinal axis, with shadowing stones in the neck of the gallbladder, a thickened wall, and complex fluid in the gallbladder fossa. Image b shows the gallbladder in transverse view and again shows the complex fluid and soft tissue changes in the gallbladder fossa alongside the liver. Image c shows a longitudinal view of the gallbladder with hyperemia in the gallbladder wall abutting the gallbladder fossa, as depicted by color flow doppler.
72365c01 gallbladder wall fluid in gallbladder fossa positive sonographic Murphy’s sign inflammation mechanical obstruction infection hyperemia hypervascularity dx acute calculous cholecystiis Davidoff MD |

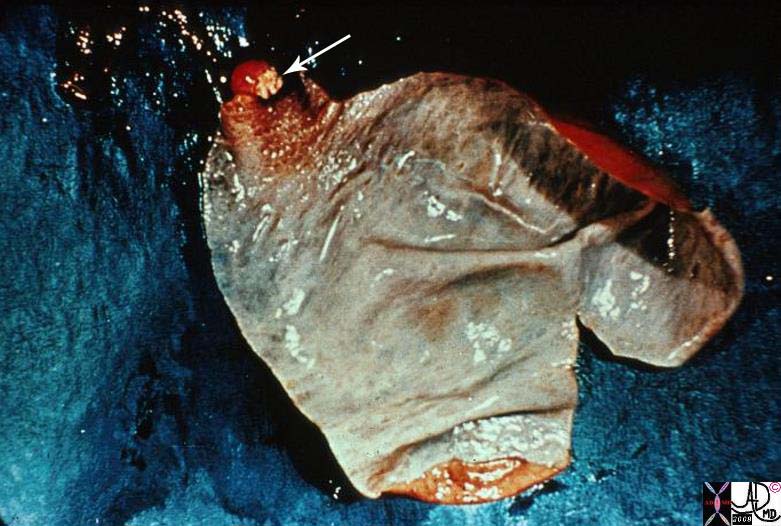
Acute Calculous Cholecystitis |
|
This is a photograph of a resected gallbladder opened longitudinally. The gallbladder is being held open by hemostats, as the inflammatory process made the wall thicker and stiffer than normal. Note that the cut face of the wall between the hemostats is about 3 – 4 mm thick. The dark red color is imparted by hemorrhage in the wall. The multiple gallstones are probably causing some degree of obstruction. 11927.8s gallbladder cholecytitis grosspathology Courtesy Barbara Banner MD |
Fluid and Thickening in the Gallbladder Fossa |
|
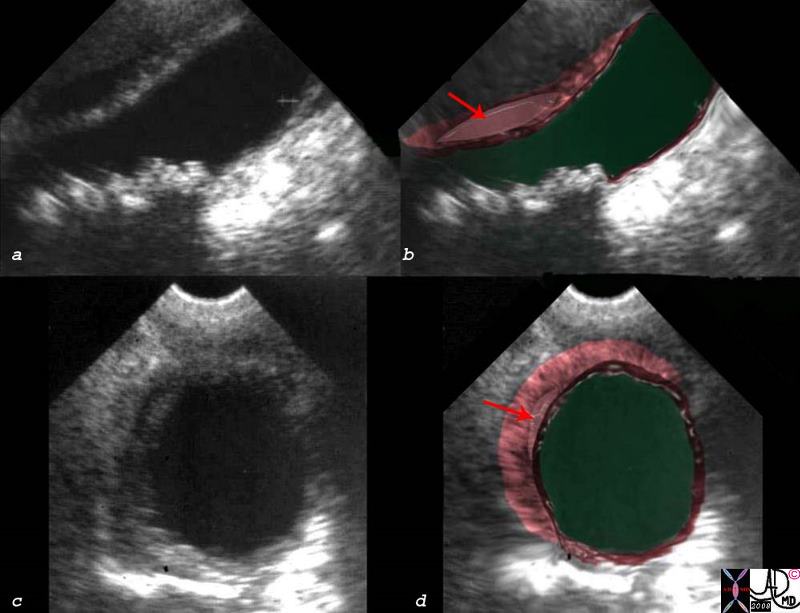
The patient presented with right upper quadrant pain RUQ pain, positive Murphy’s sign, fluid in the gallbladder fossa (red arrow in b and d)thickened linear lacy thickening (dark pink) and small shadowing stones (a,b) The diagnosis is consistent with acute cholecystitis. acute calculous cholecystitis USscan ultrasound Courtesy Ashley Davidoff MD copyright 2008 00543c03s.8 |
The accumulation of fluid in this area make blunt dissection for the surgeon relatively easy and surgeons say that if it is present they can use their fingers to dissect the gallbladder from the liver
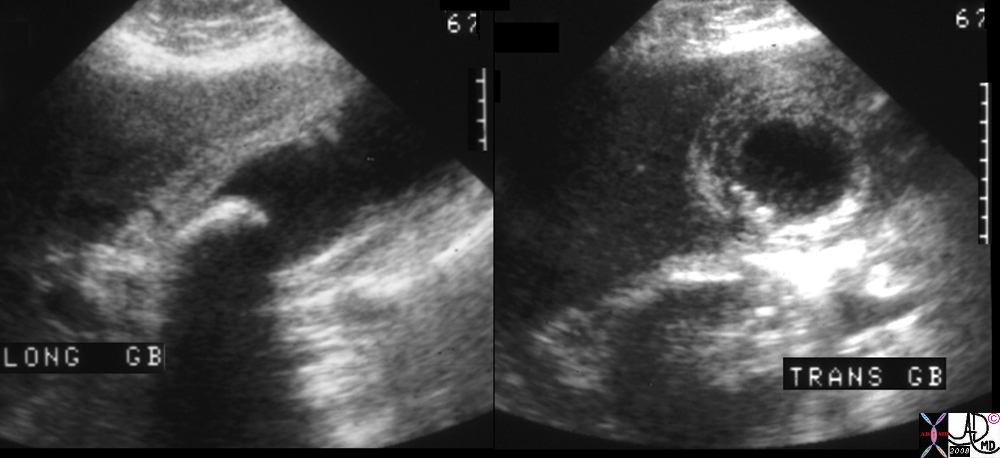 Acute Cholecystitis00401.1cs 67Male right upper quadrant pain RUQ pain positive Murphy’s sign gallbladder gallbladder fossa thickened linear lacy thickening gall stones calculi calculous large stone in the infundibulum shadowing multiple small stones cholelithiasis cholecystitis acute cholecystitis acute calculous cholecystitis USscan ultrasound Courtesy Ashley Davidoff MD copyright 2008
Acute Cholecystitis00401.1cs 67Male right upper quadrant pain RUQ pain positive Murphy’s sign gallbladder gallbladder fossa thickened linear lacy thickening gall stones calculi calculous large stone in the infundibulum shadowing multiple small stones cholelithiasis cholecystitis acute cholecystitis acute calculous cholecystitis USscan ultrasound Courtesy Ashley Davidoff MD copyright 2008
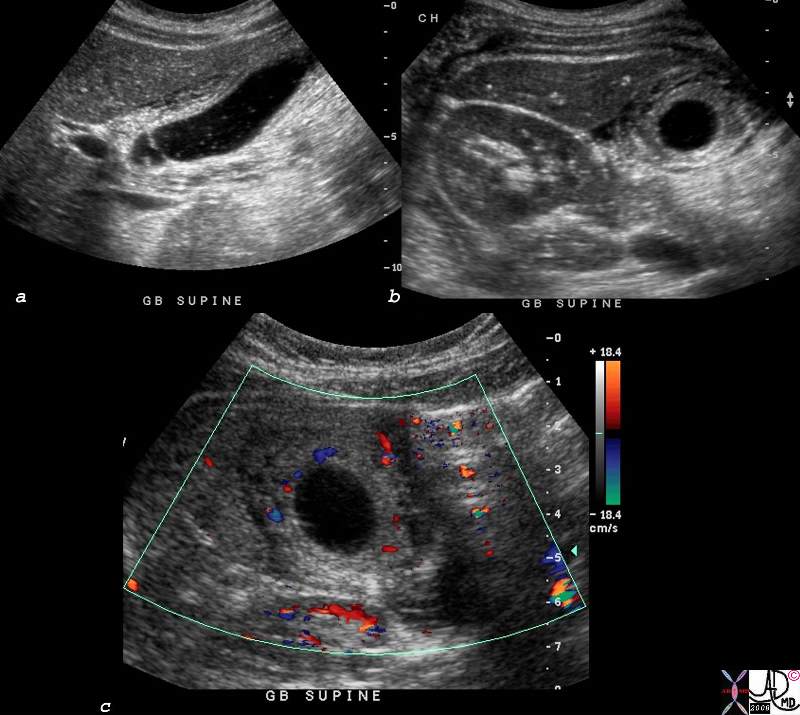
 Acute Cholecystitis Caused by Cholesterol Crystals
Acute Cholecystitis Caused by Cholesterol Crystals
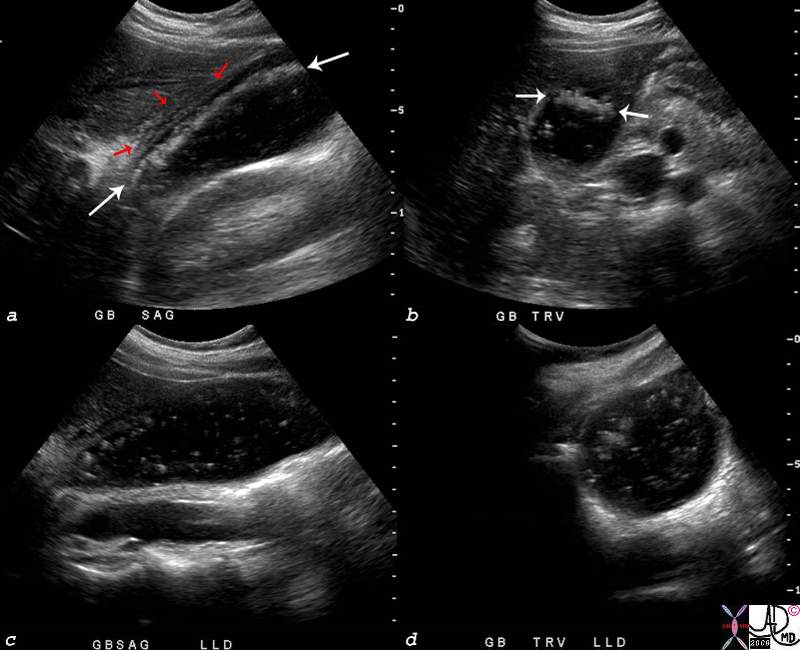
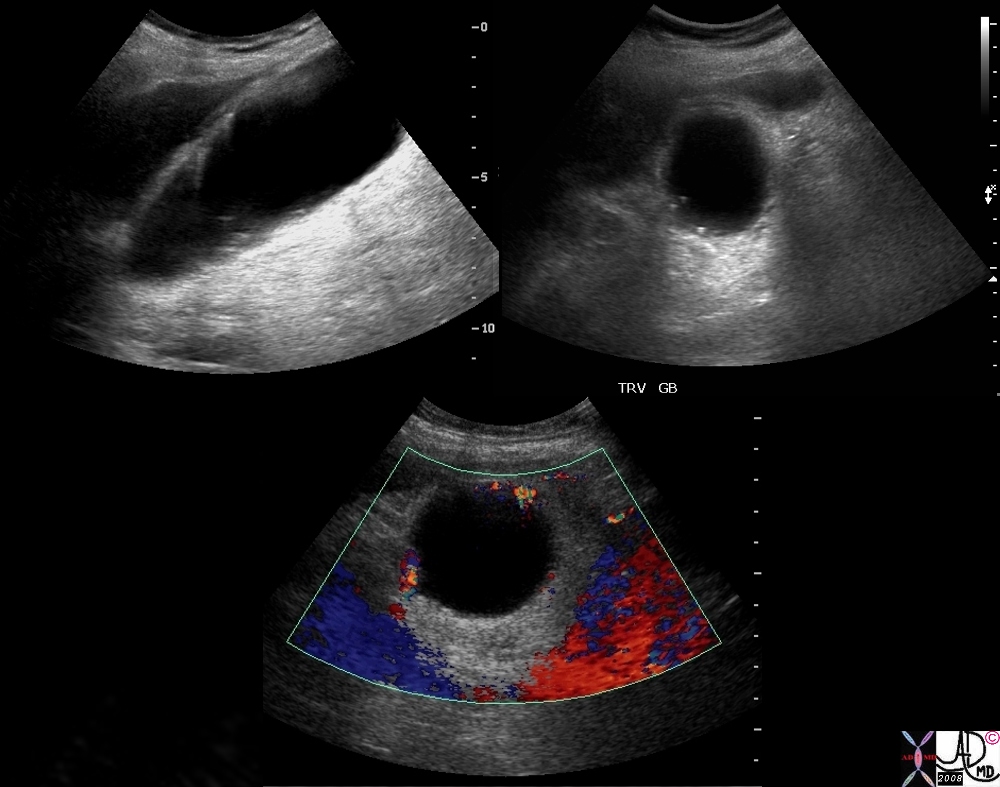
The ultrasound scan is from a young female who presented with right upper quadrant pain and positive Murphy’s sign – a clinical sign that is consistent with acute cholecystitis. The scan shows multiple floating stones (white arrows) in the longitudinal view (a) and in the transverse view (b). There are complex changes in the gallbladder fossa (red arrows) characterized by fluid and linear echoes, both characteristic of acute cholecystitis. Perturbation of the stones disturbed the layering effect and the crystals were seen floating throughout the lumen.
77753c03.8s young female right upper quadrant tenderness RUQ gallbladder echogenic irregular fluid fluid layer conforming to the shape of the gallbladder wall thickened linear echoes floaters crystalline SG less than bile cholesterol crystals specific gravity forces space cholelithiasis stones small acute cholecystitis USscan ultrasound Courtesy Ashley Davidoff MD For Radiologists and Detectives
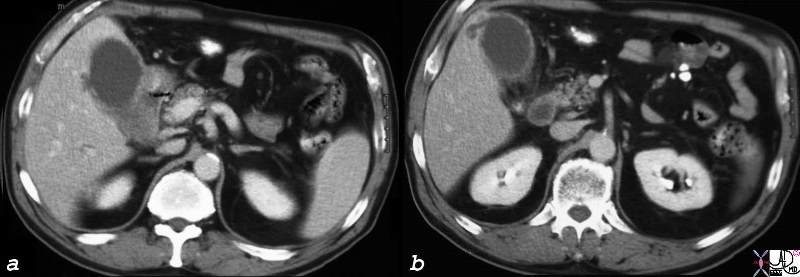
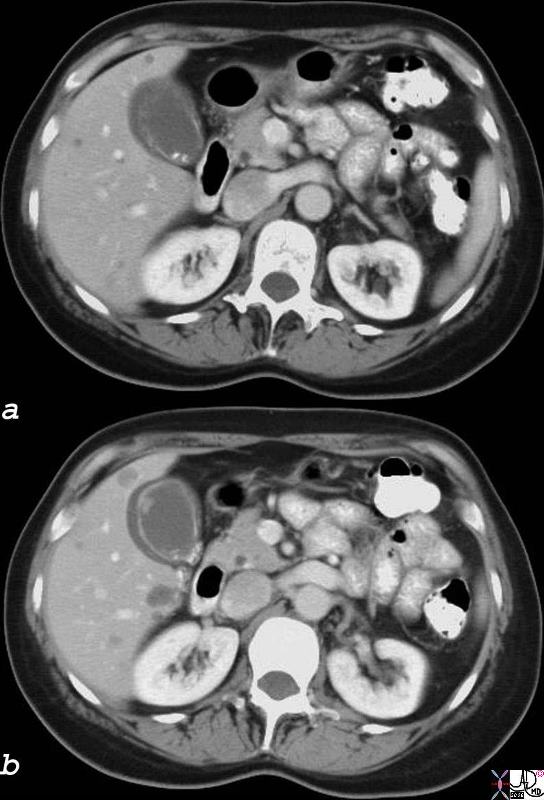 Acute Cholecystitis with Fluid in the Gallbladder Fossa 18333c01.8s gallbladder edematous wall hyperemic wall distended gall bladder edema in the wall fluid in the gallbladder fossa GBF fluid acute cholecystitis stones visible on CT scan cholelithiasis gallbladder polyp CTscan Courtesy Ashley Davidoff MD copyright 2008
Acute Cholecystitis with Fluid in the Gallbladder Fossa 18333c01.8s gallbladder edematous wall hyperemic wall distended gall bladder edema in the wall fluid in the gallbladder fossa GBF fluid acute cholecystitis stones visible on CT scan cholelithiasis gallbladder polyp CTscan Courtesy Ashley Davidoff MD copyright 2008
Spread of disease via the Gallbladder Fossa
If there is a superadded infection, spread to the gallbladder fossa and directly to the liver is the obvious route via the lymphatics and veins. The same holds true for the spread of gallbladder cancer – ie directly into the liver.
Eccentric thickening of the gall bladder fossa also occurs in patients with hepatitis, presumably due to increased lymphatic pressure in the liver as a result of the inflammation and thus impedance of lymphatic drainage from the gallbladder
Liver Abscess
Cholecystitis Complicated by Abscess Formation in the Gallbladder Fossa
The artistic rendition shows 2 stones lying free in the lumen and one impacted in the neck of the gallbladder with secondary inflammatory changes in the wall(red) and abscess formation in the gallbladder fossa and extension into the neighbouring liver.
11921.8b05b037.8s gallbladder cystic duct gallstones cholelithiasis stone impacted in the cystic duct distended enlarged hyperemic wall complex fluid in the gallbladder fossa tumefactive bile cholestasis sludge acute cholecystitis abscess formation Davidoff Art copyright 2008
 Early Abscess Formation16188c05.8 gallbladder hyperemic thickened wall early abscess formation fluid collections in the gallbladder fossa acute cholecystitis CTscan Courtesy Ashley Davidoff MD copyright 2008
Early Abscess Formation16188c05.8 gallbladder hyperemic thickened wall early abscess formation fluid collections in the gallbladder fossa acute cholecystitis CTscan Courtesy Ashley Davidoff MD copyright 2008
Acute Cholecystitis |
|
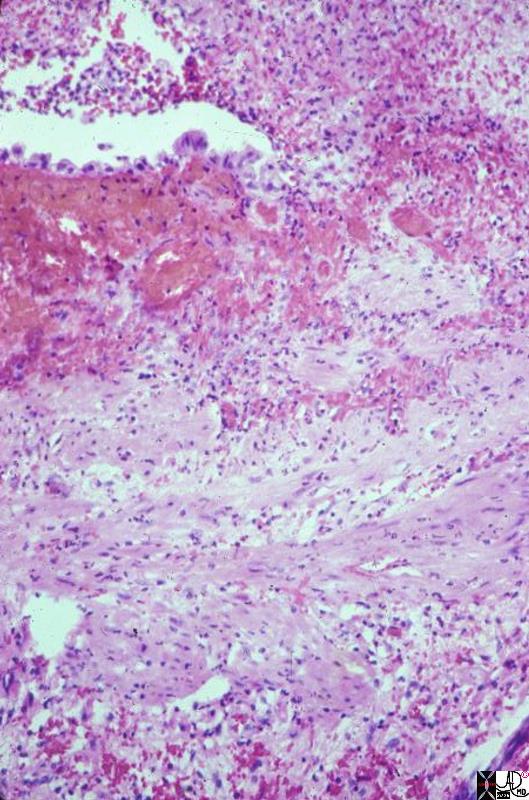
This is a high power photomicrograph of mucosa and muscular layer of a gallbladder with acute cholecystitis. Just a bit of the lumen is shown, indicated by the empty slit at one side of the picture. The fronds are flat, and a single layer of epithelium can be seen (at the edge of the slit). The epithelium is interrupted by acute inflammatory exudate which is extruding from the mucosa into the lumen. Hemorrhage is present beneath the epithelium, and there is acute inflammation through the wall. 11926.8s gallbladder cholecyctitis pathology histopathology Courtesy Barbara Banner MD |
Acute Cholecystitis |
|
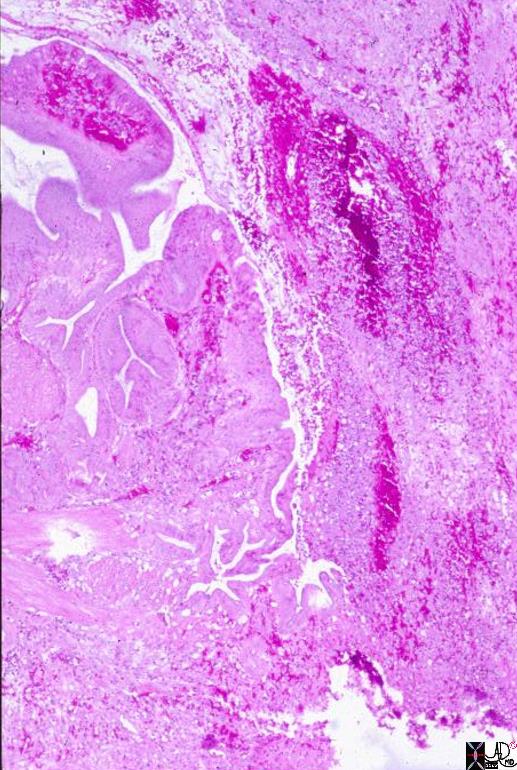
This low power photomicrograph indicates how Rokitansky-Aschoff sinuses provide a route for perforation. Here full thickness of the wall is shown. The fronds can be identified on one side, projecting into lumen, shown in the corner of the picture. in the center, the fronds turn down and project out through the muscular layer. This is the Rokitansky-Aschoff sinus. The other half of the picture consists of acute inflammatory exudate mixed with hemorrhage extending from the lumen out through the Rokitansky-Aschoff sinus. 11929b.8s gallbladder cholecystitis histopathology Courtesy Barbara Banner MD |
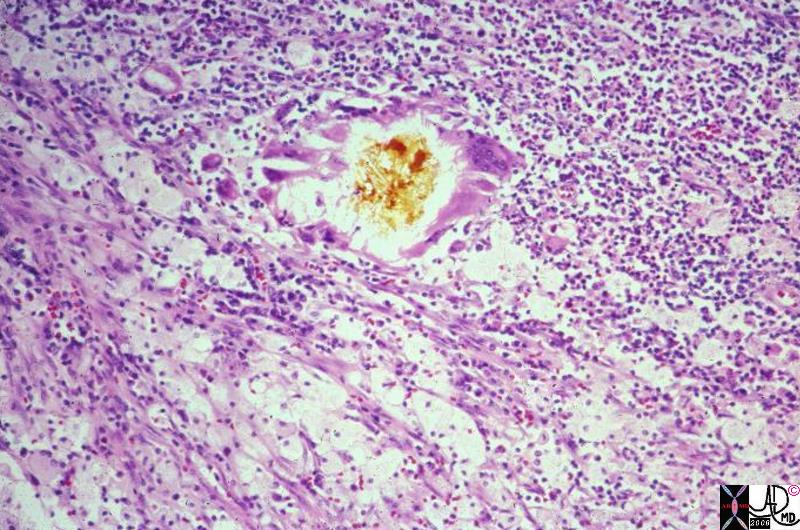
Pathogenesis of Acute Cholecystitis |
|
This is a low power photomicrograph showing mucosal fronds. The empty part of the picture is the gallbladder lumen, and the serosa, not seen here, would be on the opposite side of the gallbladder. Acute cholecystitis begins as an area of chemical injury to the mucosa. The trigger for this injury is not always clear, but in many cases obstruction of the neck or cystic duct by stone or sludge is present. As the gallbladder distends there is diminution of blood flow. Anoxia makes the epithelium more susceptible to injury from the retained bile components. Here a discrete focus of necrosis can be seen as the yellow, bile-stained, infarct-like area of mucosa in the center of the picture. Inflammation is present, but not easily seen at this magnification. Early in acute cholecystitis, chemical/anoxic injury is out of proportion to the amount of inflammation. Inflammation progresses, however, and if this gallbladder had been resected a day later, we would see many more inflammatory cells throughout the wall. 11923.8s gallbladder cholecystitis pathology histopathology Courtesy Barbara Banner MD |
Pathogenesis of Acute Cholecystitis |
|
This is a medium power photomicrograph of the mucosa in a gallbladder with acute cholecystitis. The early changes involve chemical injury from bile components exacerbated by anoxia created as the gallbladder distends and small vessels are compressed. Here a bile-stained infarct-like area of necrosis is seen with ghosts of the normal mucosal components such as stroma and vessels. An inflammatory infiltrate is present, but necrosis is the dominant feature. gallbladder cholecystitis pathology histopathology Courtesy Barbara Banner MD 11924.8s |
Bile Inciting Inflammation |
|
This photomicrograph shows a small piece of bile, in its yellow natural color, surrounded by foreign body type giant cells, surrounded in turn by a sea of WBCs and foamy histiocytes. The latter contain bile and lipid salts. The bile and the foamy histiocytes account for the yellow color seen grossly in xanthogranulomatous cholecystitis. The “granulomas” are true foreign body-type granulomas composed of phagocytes trying to break down chunks of bile which have worked their way into the gallbladder wall during inflammatory disruption of the mucosa. 11938.8 gallbladder dx cholelithiasis histopathology Courtesy Barbara Banner MD |
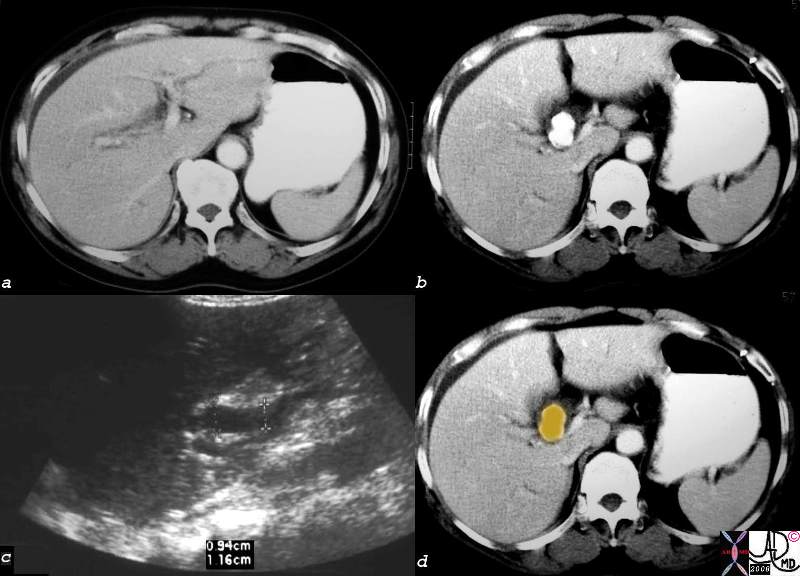
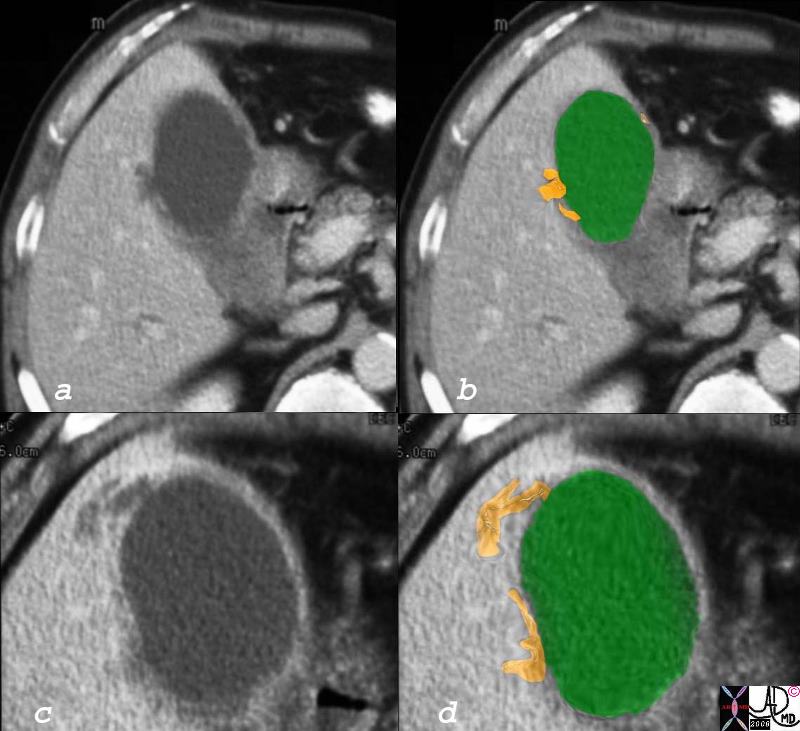
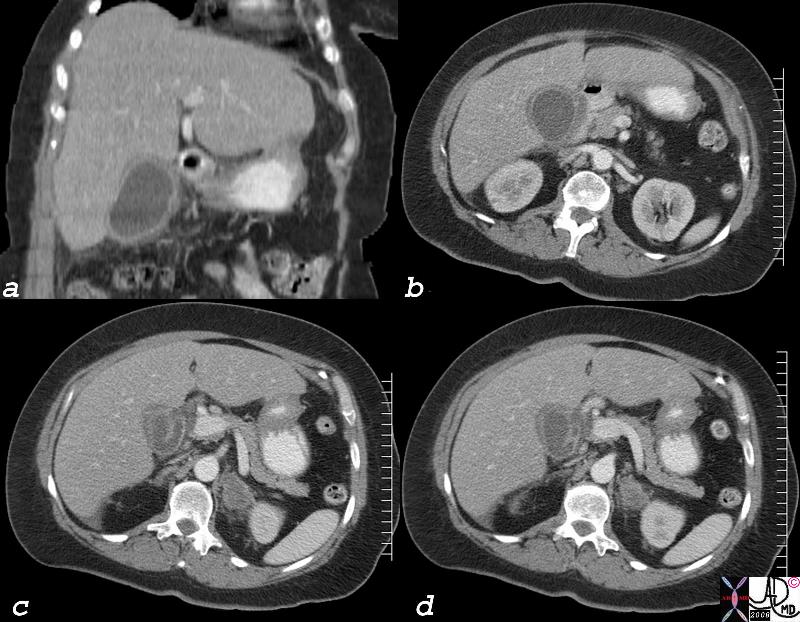
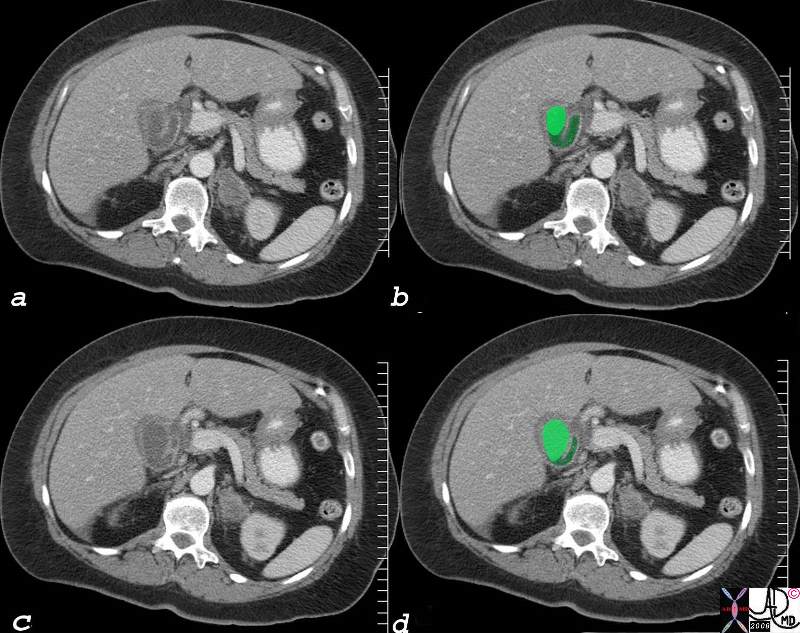
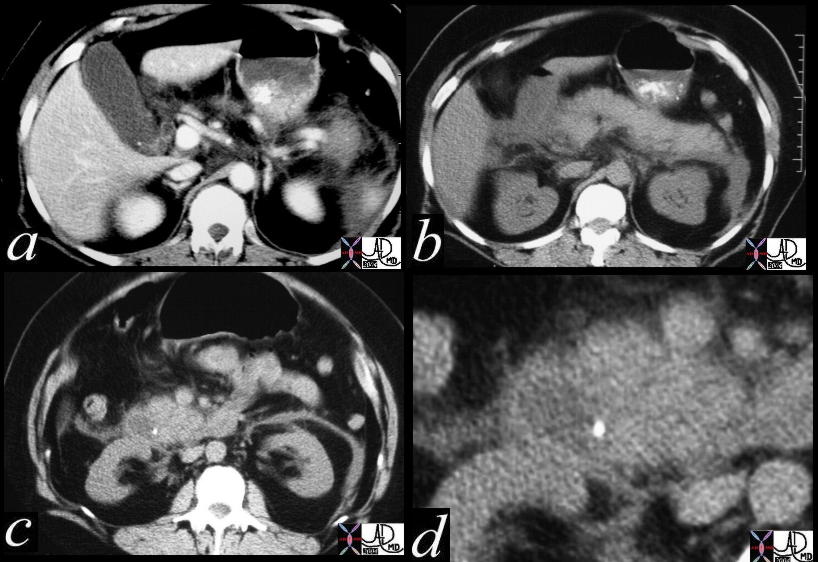
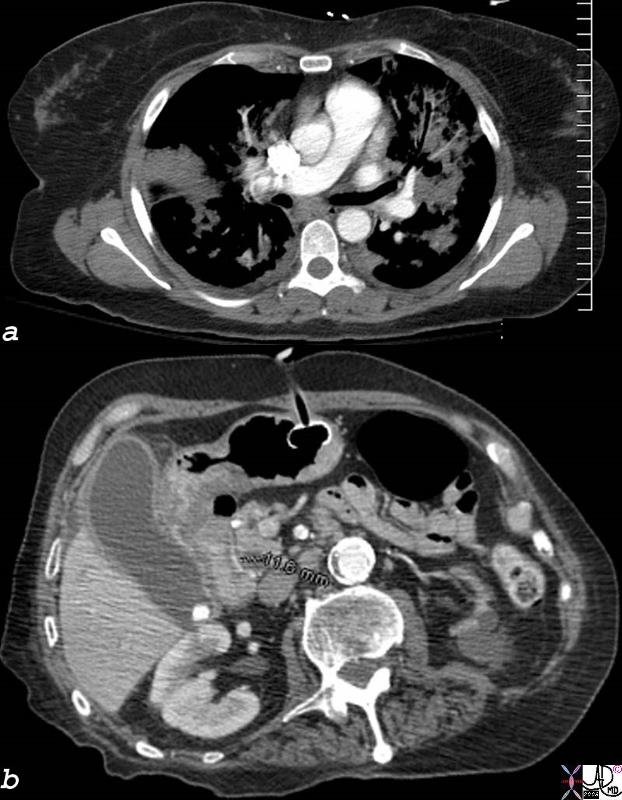
Mirizzi’s Syndrome – Large Stone in the Infundibulum Bile Duct Obstruction |
| 57year old male presents with RUQ pain fever, positive Murphy’s sign, elevated alkaline phosphatase. The CTscan in a shows mild intrahepatic bile duct dilatation, while image b shows a 2.8cms stone impacted in the region of the infundibulum of the gallbladder. Image c is an ultrasound which shows dilated common hepatic duct (up to 1.2cms) while d shows an overlay in orange of the gallstone. At surgery the stone was noted to be impacted in an Hartmann’s pouch. The combination of acute cholecystitis with bile duct obstruction caused by mass effect of a stone in the base of the gallbladder causing extrinsic compression is called Mirizzi’s syndrome.
gallbladder stone cholelithiasis cholecystitis bile duct obstruction Mirizzi’s syndrome USscan ultrasound CTscan Courtesy Ashley Davidoff MD copyright 2008 82342c.8s |

Interscapular Pain |
|
The pain does sometimes radiate to the infrascapular region or to the back. 49640c03 chest back pain belt interscapular band like pancreas gallbladder retroperitoneum retroperitoneal structures CTscan Courtesy Ashley Davidoff MD 3D |
|
Hyperplastic Cholecystosis with Acute Cholecystitis filled with stones in the Fundus |
|
In this ultrasound of the gallbladder is from a patient with right upper quadrant pain the gallbladder in the transverse plane measures 5cms and is round in shape rather than oval. The diagnosis was acute cholecystitis. 78434c01s right upper quadrant pain positive Murphy’s sign gallbladder outpouchings diverticula prominent Aschoff Rokitansky stones ring down artifact thickened wall hyperemic wall by doppler hyperplastic cholecystosis hyperplastic cholecystoses adenomyomatosis acute cholecystitis USscan ultrasound courtesy Ashley Davidoff MD copyright 2008 |
BACKGROUND TO THE DISEASE:
Gallstone disease affects 10-20% of the population, though the majority are asymptomatic incidental findings. Classically occur in fair, fat, fertile females in their forties – fifties. Most gallstones are predominantly cholesterol (80%, often solitary if solely cholesterol), but may also be pigmented (formed from bile with less than 25% cholesterol content, usually multiple and irregular) or mixed (faceted appearance, calcium containing). 90% of patients who develop acute cholecystitis have gallstones. Symptoms typically follow impaction of a gallstone in the cystic duct. It is differentiated from biliary colic mainly by the presence of inflammation (fever, leucocytosis, local peritonism); also the pain is not necessarily associated with food.
Dilated Cystic Duct |
| 77742c01.8s gallbladder distended enlarged pericholecystic fluid fluid in the gallbladder fossa gbf cystic duct enlarged dilatation of the cystic duct acute cholecystitis adremnal metastasis CTscan Courtesy Ashley Davidoff MD copyright 2008 |
Dilated Cystic Duct |
| 77742c03.8s gallbladder distended enlarged pericholecystic fluid fluid in the gallbladder fossa gbf cystic duct enlarged dilatation of the cystic duct acute cholecystitis adremnal metastasis CTscan Courtesy Ashley Davidoff MD copyright 2008 |
Dilated Cystic Duct CBD stone |
| 16225c Courtesy Ashley Davidoff MD code gallbladder + infundibulum fx calcification dx cholelithiasis code cystic duct fx dilated fx enhancingwall dx obstruction code abdomen retroperitoneum Gerota’s fascia fx indurated code pancreas pancreatic uncinate process fx indurated bile duct fx dilated fx enhancing wall fx calcification stone dx choledocholithiasis dx gallstone pancreatitis + imaging radiology CTscan |
 Gallbladder Filled with Stones Gallbladder Filled with Stones |
| 77744c01.8s gallbladder distended enlarged pericholecystic fluid fluid in the gallbladder fossa wall thickened hyperemic almost completely filled with stones shadowing cholellithiasis hypervascular gbf acute cholecystitis USscan ultrasound color flow doppler Courtesy Ashley Davidoff MD copyright 2008 |
 Acute on Chronic Cholecystitis Acute on Chronic Cholecystitis |
| 81983c01.8s 31 F pw abdominal pain chronic cholecystitis cholelithiasis at path fluid was gelatinous green cholesterol choleliths measuring up to 6mm focal congestion of mucosa cystic duct occluded with 9mm mulberry cholesterol stone gallbladder thick wall hyperemic cholesterol crystals complex fluid in the gallbaldder fossa GBF dx acute on chronic cholecystitis USscan ultrasound color flow doppler Courtesy Ashley Davidoff MD copyright 2008 |

Acute Cholecystitis with denuded Mucosa |
| 78371c02.8s middle aged male with right upper quadrant pain RUQ pain gallbladder shadowing stones distended gallbladder denuded mucosa USscan ultrasound Courtesy Ashley Davidoff MD copyright 2008 |
CLINICAL BACKGROUND –
The “classical ” presentation of acute cholecystitis is characterised by intermittant RUQ pain that lasts for 1-6 hours with intermittant colicky components when the intensity of the pain increases. Precipitaing factors include a recent ingestion of a meal.. The pain may radiate to the right scapula or shoulder. Associated symptoms include nausea and vomiting, fever and chills. While the wcc is usually elevated, a normal wcc does not exclude the diagnosis. The bilirubin and alakaline phosphatase are usually slightly elevated. Murphy’s sign is diagnostic.
 Acalculous or Calculous Cholecystitis? Acalculous or Calculous Cholecystitis? |
| 78335c01.8s elderly female in ICU setting with pneumonia and ARDS and gastrostomy feeding tube. CTscan shows gallbladder distended and enlarged hyperemic thickened wall induration in the fat around the gallbladder gall stone cholelithiasis differential diagnosis includes acaclculous cholecystitis and calculous cholecystitis CTscan Courtesy Ashley DAvidoff copyright 2008 |
IMAGING STRATEGIES
WHAT STUDY?
Ultrasound is the investigation of choice in this patient with suspected acute cholecystitis. Findings of a probe tender, distended gallbladder, with fluid in the gallbladder fossa and gallstones are pathognomonic features. Plain abdominal film is not helpful in the diagnosis. In the equivocal case when ultrasound is not characteristic and the clinical suspicion is strong, an imaging alternative is a HIDA scan.
Ultrasound provides a non-invasive method for establishing evidence of gallstones / gallbladder inflammation as a cause for the symptoms. Acute cholecystitis is an indication for cholecystectomy. If the symptoms are of less than 48 hours duration this can be performed immediately; alternatively, the gallbladder may be removed after the inflammation has settled in 4-6 weeks (interval cholecystectomy). Ultrasound should be performed at time of presentation, as the patient requires immediate management.
The most sensitive examination for acute cholecystitis is the HIDA scan which when normal will show the gallbladder filling approximately 30-60 minutes following technetium injection. If the gallbladder does not fill it correctly implies that the cystic duct is obstructed. In the appropriate clinical setting the lack of filling of the gallbladder is pathognomonic for acute cholecystitis.
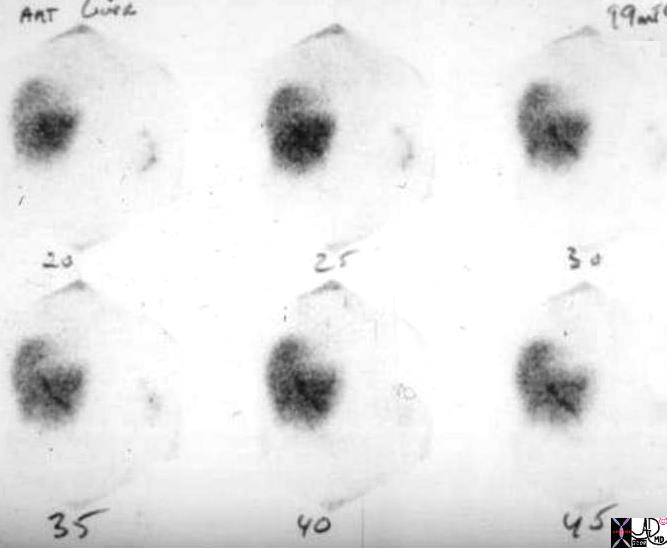
 Stone Impacted in the neck Positive HIDA scan Stone Impacted in the neck Positive HIDA scan |
| This young patient presented with right upper quadrant pain and shows a fairly large stone impacted in the infundibulum on the longitudinal view of the ultrasound. Fluid is also noted in the gallbladder fossa. The HIDA scan shows non visualization of the gallbladder at 60 minutes, despite the filling of the small bowel. These findings are consistent with the diagnosis of acute cholecystitis.
78306c01.8s young female vague right upper quadrant pain non distended gallbladder complex fluid in the gallbladder fossa large stone cholelithiasis non visualization non viz radioactive labelled technetium HIDA scan non visualization of the gallbladder at 45 minutes biliary system visualized at 30 minutes consistent with acute cholecystitis nuclear medicine Courtesy Ashley Davidoff MD copyright 2008 |
Positive HIDA scan |
| 04505bs radioactive labelled technetium HIDA scan non visualization of the gallbladder at 45 minutes biliary system visualized at 30 minutes consistent with acute cholecystitis nuclear medicine Courtesy Ashley Davidoff MD copyright 2008 |
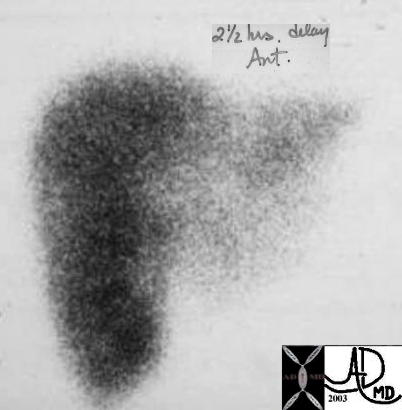
HIDA scan Positive for Acute Cholecystitis |
| The scan was taken at 2 and half hours after administration of the radiosotope, and fails to show filling of the gallbladder. This finding confirmins an obstruction of the cystic duct and the diagnosis of acute cholecystitis is highly likely.
04208 gallbladder non-filling HIDA scan dx acute cholecystitis imaging radiology nuclear medicine NMscan |
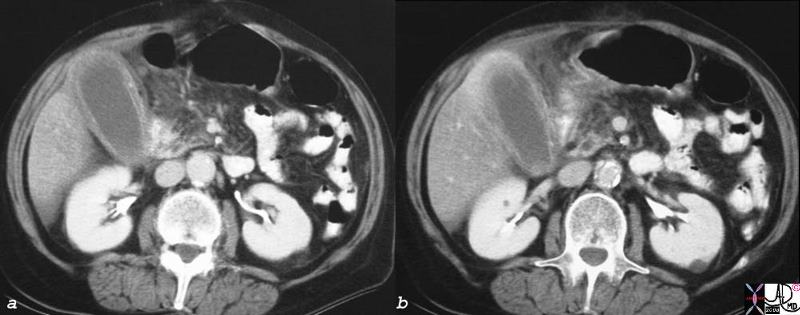
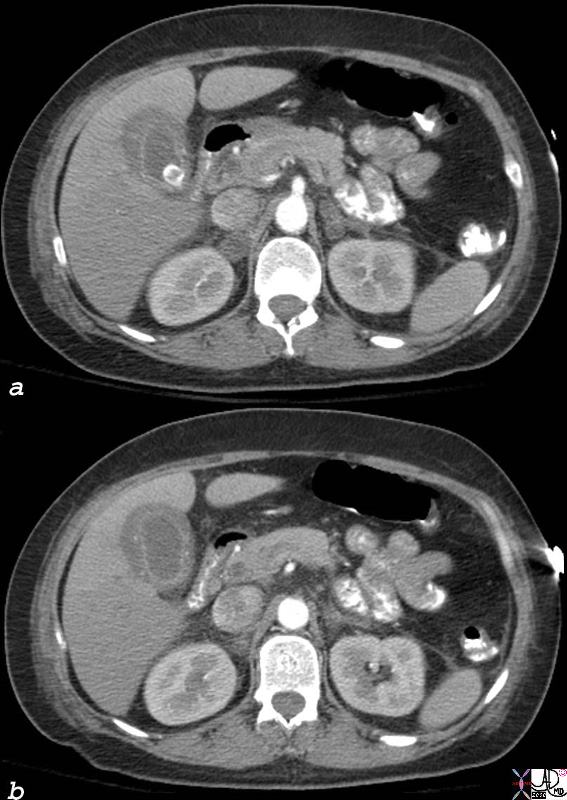
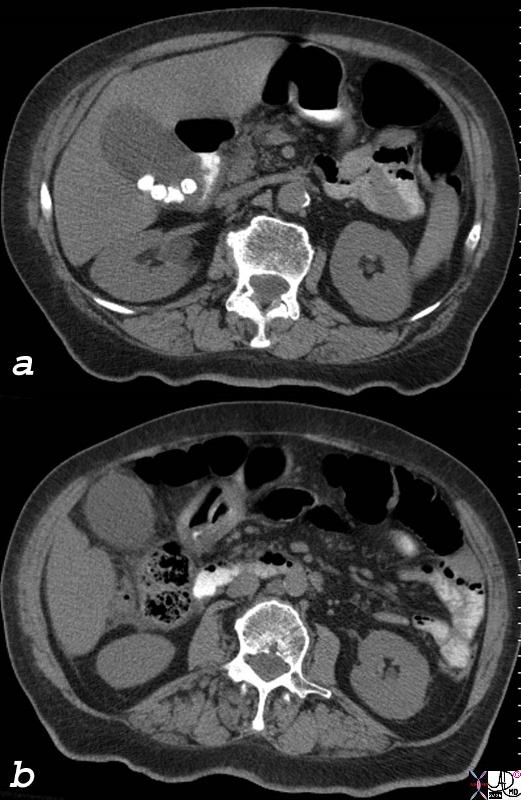 Acute Calculous Cholecystitis Acute Calculous Cholecystitis |
| 77728c01.8s gallbladder edematous wall distended gall bladder edema in the wall fluid in the fat surrounding the gallbladder indurated fat acute cholecystitis calcified stones cholelithiasis stones visible on CT scan CTscan Courtesy Ashley Davidoff MD copyright 2008 |
If the inflammation and ischemia are ongoing the wall breaks down and transudation or leakage of fluid occurs in the pericholecystic fat. This is best visualized by CT scan. This finding suggests an advanced form of the disease and treatment becomes emergent.
|
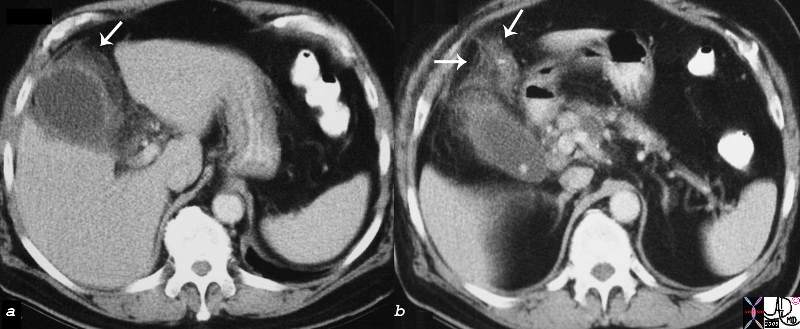
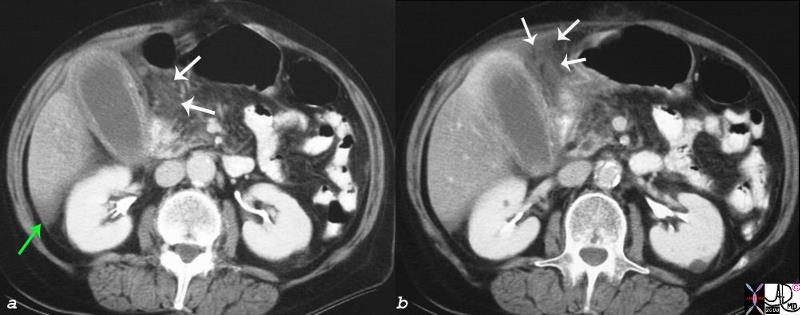
16157c03.8s gallbladder edematous wall distended gall bladder edema in the wall fluid in the fat surrounding the gallbladder indurated fat free fluid in Morrison’s pouch acute cholecystitis stones not visible on CT scan CTscan Courtesy Ashley Davidoff MD copyright 2008 |
Acute Cholecystitis with Adenomyomatosis |
| 78434c02s right upper quadrant pain positive Murphy’s sign gallbladder outpouchings diverticula prominent Aschoff Rokitansky stones ring down artifact thickened wall hyperemic wall by doppler hyperplastic cholecystosis hyperplastic cholecystoses adenomyomatosis acute cholecystitis USscan ultrasound courtesy Ashley Davidoff MD copyright 2008 |
Acute Cholecystitis with Adenomyomatosis |
| 82109c01.8s gallbladder adenomyomatosis stones calcifications in the wall thickened wall edematous wall hyperplastic cholecystoses calcifications stones thickened wall edema acute cholecystitis Aschoff-Rokitansky sinuses CTscan Courtesy Ashley Davidoff MD copyright 2008 |
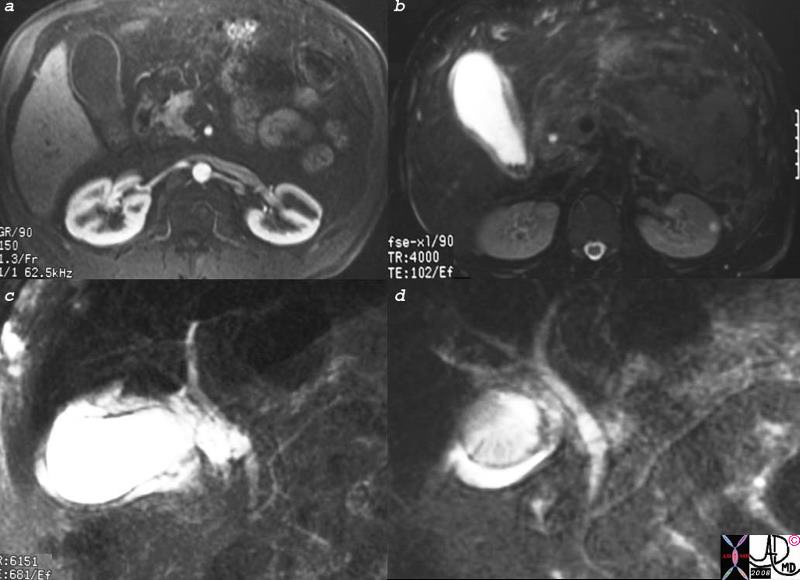
Acute Cholecystitis |
| 16141c01s.8 gallbladder stones cholelithiasis hyperemic wall edematous wall small filling defects in dependant position in the infundibulum distended gall bladder edema in the wall fluid in the gallbladder fossa gbf normal bile duct MRI T1 weighted image with gadolinium and fat saturation T2 weighted MRCP normal pancreatic duct Courtesy Ashley Davidoff MD copyright 2008 |
|
Acute Cholecystitis |
| 16141c01s.8 gallbladder stones cholelithiasis hyperemic wall edematous wall small filling defects in dependant position in the infundibulum distended gall bladder edema in the wall fluid in the gallbladder fossa gbf normal bile duct MRI T1 weighted image with gadolinium and fat saturation T2 weighted MRCP normal pancreatic duct Courtesy Ashley Davidoff MD copyright 2008 |
Complications
A second complication to consider is not as common is abscess formation which most commonly occurs in the gallbladder fossa. The fluid that has collected in the gallbladder fossa becomes secondarily infected and an abscess forms. This needs to be drained and percutaneous techniques are best suited to do this.
Early Abscess Formation |
| 16188c.8s gallbladder hyperemic thickened wall early abscess formation fluid collections in the gallbladder fossa acute cholecystitis CTscan Courtesy Ashley Davidoff MD copyright 2008 |
 Chronic Impaction – Hydrops of the Gallbladder Chronic Impaction – Hydrops of the Gallbladder |
| This is a gross photograph of a gallbladder opened longitudinally to show the mucosal surface. The gallbladder is distended, and its walls are very thin. Look carefully and note part of a light tan, granular gallstone protruding from the neck of this gallbladder, where it is impacted. This impaction has obstructed the gallbladder, preventing bile from getting in from the liver. The columnar cells lining the gallbladder keep producing mucin, their normal function, and the mucin cannot exit the gallbladder. Therefore, the gallbladder gets progressively distended with a clear, glairy mucin, and this situation is called hydrops of the gallbladder.
11917.8s01 gallbladder dx cholelithiasis grosspathology Courtesy Barbara Banner MD |
Treatment
 Acute Cholecystitis Treated with Cholecystostomy Acute Cholecystitis Treated with Cholecystostomy |
| 78304c01.8s elderly lady with multiple comorbid ilnnesses presents with RUQ pain fever, positive Murphy’s sign gallbladder distended cholelithiasis shadowing hyperemic wall complex fluid in the gallbladder fossa GBF stones acute cholelcystitis percutaneous cholecystostomy pigtail minimally invasive therapy MIT USscan ultrasound doppler color flow Courtesy Ashley Davidoff MD copyright 2008 |
The patient for US should be fasting for 4 hours and the study should take about thirty minutes.
CLINICAL RED FLAGS:
A triad of jaundice, fever and RUQ pain (Charcot’s triad) is indicative of cholangitis, which has a high mortality if not treated promptly with appropriate antimicrobials (to cover enterococcus and enteric organisms, typically 3rd generation cephalosporin and metronidazole). Acalculous cholecystitis, in which no gallstones are visualized, may be seen in the elderly, trauma, or ICU setting and also has a high mortality without treatment.
Web References
ACR
Acute Abdominal Pain and Fever
Acute Right Upper Quadrant Pain
American Society of Gastroenterology