
Definition
Gallbladder carcinoma is a malignant disease usually originating in the epithelium lining. Its cause is unknown, but the high incidence of associated cholesterol gallstones (>75%) creates an etiological link between the two diseases.
Tumors of the biliary system are found mostly in the elderly in the seventh decade of life and are 3-4 times as common in women as in men. It is strongly associated with gallstones, but while nearly 80% of those with carcinoma have concomitant gallstones, less than 0.5% of all patients with gallstones will develop carcinoma. Porcelain gallbladder predisposes to the development of carcinoma.(25% incidence)
Structurally it can present with focal thickening of the wall, polypoid lesion, or a mass, and is most common in the fundus (60%) , followed by the body 30%, and then the neck (10%).
Functional impairment is limited and it is for this reason that presentation is late and prognosis is poor.
Complications include early spread to the regional nodes and direct invasion into the liver through the gallbladder fossa.
Clinically the patient usually presents late in the disease with symptoms similar to that of cholelithiasis. RUQ pain, jaundice, and nausea with vomiting. Occasionally this results in a palpable gallbladder before invasion into the adjacent structures. Still, it is rarely found at a time when surgical resection is possible, and thus has a 5-year survival rate of ~1%.
The diagnosis is rarely suspected given the above symptoms, and is often only found incidentally on resection of a gallbladader for symptomatic cholelithiasis.
From an imaging standpoint, ultrasonography will often reveal a thickened wall or polypoid masses, though these features may not specific for carcinoma. A polyp that is larger than 1cms is suspicious for carcinoma. CT may also identify a mass or thickening within the gallbladder, but the diagnosis is usually suggested when spread to the liver adjacent to the gallbladder fossa is identified or when regional adenopathy is present. Magnetic resonance cholangiopancreatogrphy may also help visualize the liver, biliary treee and neighboring lymph nodes but offers no clinical advantages over CT scan.
Surgical treatment is provides the only opportunity for cure but only a minority of patients are candidates. Patients who have a porcelain gall;bladdder should have elective cholecystectomy because of the high incidence of gallbladder cancer. The role of adjuvant chemotherapy following surgery is to control microscopic disease. Role of radiation therapy is unclear.
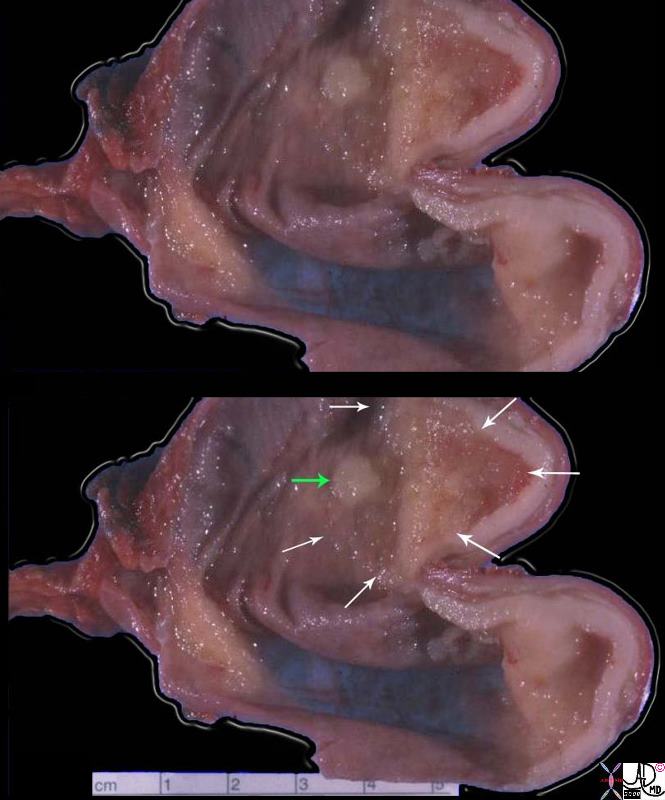 Carcinoma Thickening and Granular Appearance Carcinoma Thickening and Granular Appearance |
| This is a resected gallbladder cut longitudinally and opened like a book. You are looking into the lumen in the two halves created by the cut. The cystic duct is over the left side of the label, and the fundus of the gallbladder is over the right side. The tumor is in the fundus as tan-white tissue thickening the wall, and causing a granular appearance in the mucosa. There is a separate, 0.8 cm mucosal nodule nearby. The rest of the mucosal surface is normal appearing with small ridges, and a green-brown color. The wall is only about 1 – 2 mm thick. This carcinoma was found incidentally in this gallbladder, which was removed for gallstone. Unfortunately many gallbladder carcinomas are not diagnosed early. They are either found incidentally, like this one, or they are detected after they spread, when it is too late for effective therapy.
11951c01.8s gallbadder carcinoma grosspathology Courtesy Barbara Banner MD |
Carcinoma – Mass |
|
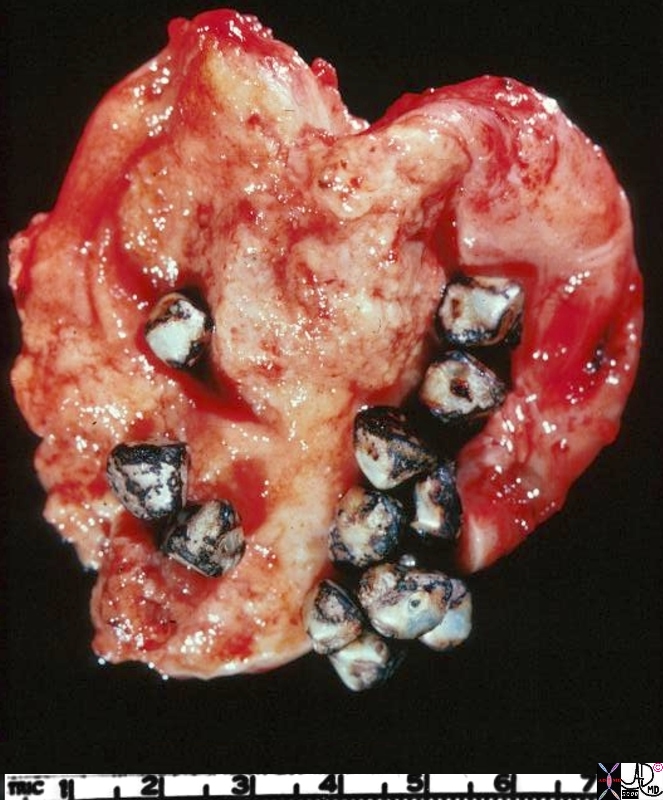
This gallbladder has been opened longitudinally and you are looking at the mucosal surface. Gallstones are present. Notice that the surface is pale tan, and irregular. The tumor produces only subtle changes in the mucosa; it is rare to have a large noticeable mass. Usually irregularity and granularity of the surface and thickening of the wall are the clues to the diagnosis. 11941.8s gallbladder carcinoma grosspathology Courtesy Barbara Banner MD |
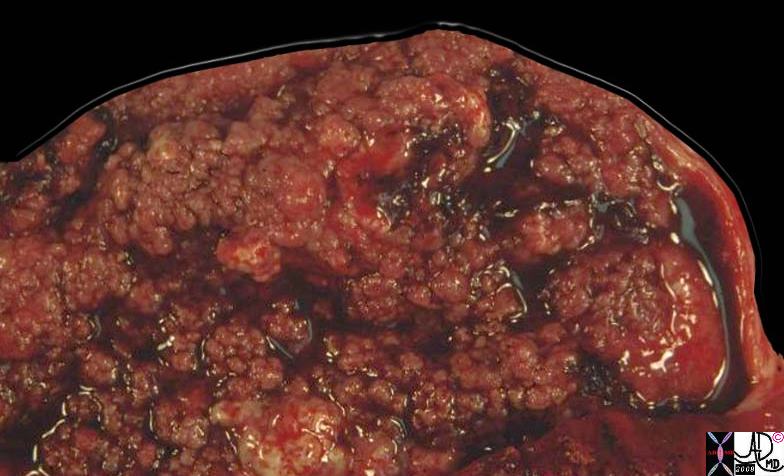
Carcinoma – Papillary Form |
|
This photograph shows a gallbladder opened so that you are looking onto the lumenal surface. The gallbladder was enlarged to the size of a grapefruit, and only about half of it is visible in this picture. The warty excresences which cover the whole lumenal surface are papillary projections of a papillary carcinoma. This carcinoma grew over the mucosal surface and into the lumen, causing the gallbladder to be greatly distended. There was no invasion of the wall itself. A small part of the wall can be seen at one side of the picture. This is an uncommon form of adenocarcinoma of the gallbladder. It is by far more common for the carcinoma to invade through the gallbladder wall. 11947.81s gallbadder carcinoma grosspathology Courtesy Barbara Banner MD |
Most exophytic carcinoma occurs in the fundus and the neck of the gallbladder.
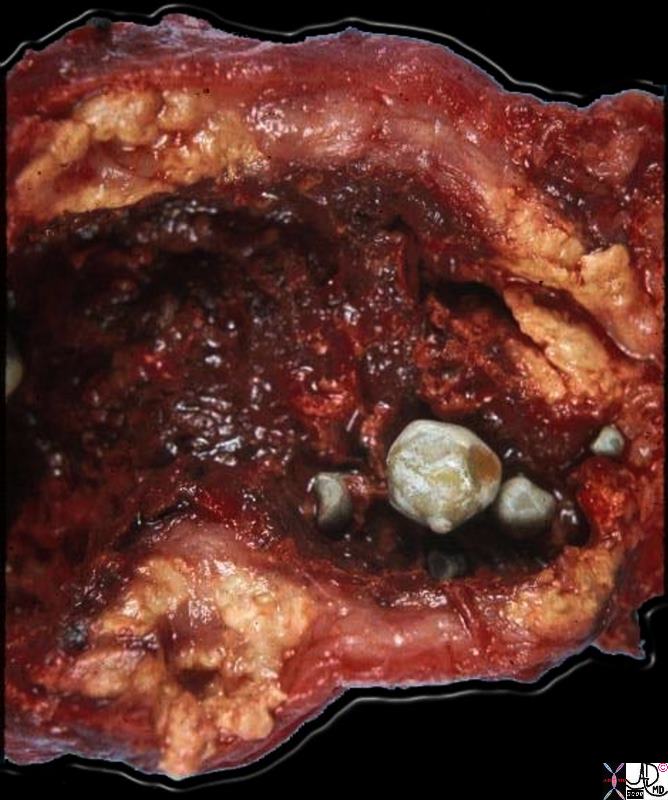
Xanthogranulomatous Cholecystitis – Acute on Chronic |
|
This gallbladder was opended longitudinally to show the lumenal surface. Four gallstones are present. The mucosal surface looks hemorrhagic, indicative of active inflammation. The most striking aspect of this gallbladder is the marked thickening and yellow color of its walls. This is due to extrusion of bile into the wall during inflammation when the integrity of the mucosa is interrupted. Once in the tissues of the wall, the bile triggers an intense inflammatory reaction, and a response by histiocytes, which phagocytose the bile and attempt to break it down. The marked accumulation of lipids and their break-down products imparts the yellow color. The significance of this variant of chronic cholecystitis is that it mimicks carcinoma by the way it thickens the wall. The radiologist, the surgeon, and even the pathologist may think this is carcinoma until the microscopic sections are examined. 11937b01.8s gallbladder dx cholelithiasis grosspathology Courtesy Barbara Banner MD |
Morphology of gallbladder carcinoma may be infitrating or exophytic. The infiltrating pattern is more common, and is characterized by deep ulcerations of the wall. These may occasionally lead to fistulous tracts forming with adjacent visceral structures, most often the liver.
82755c01.8s |
| 82755c01.8s 68 M gallbladder prone supine fundus Phrygian cap normal fundus and body are exposed to the concentrated bile normal anatomy pathophysiology Copyright 2008 Courteesy Ashley Davidoff MD |
Porcelain Gallbladder – Variant of Chronic Inflammation |
|
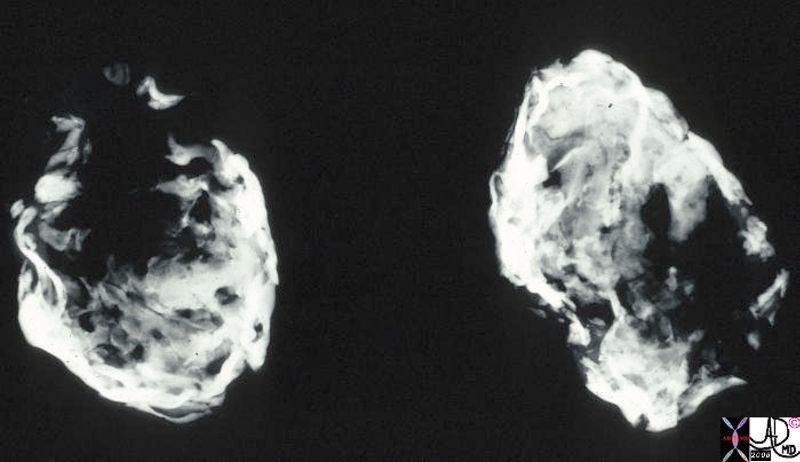
This is a specimen xray of a resected gallbladder. The walls were thin, fibrotic and heavily calcified, accounting for the radiodense (white) areas on the radiograph. This variant of chronic cholecystitis is a risk factor for development of carcinoma. 11939.8s gallbladder porcelain gallbladder X-ray Courtesy Barbara Banner MD |
Porcelain Gallbladder |
|
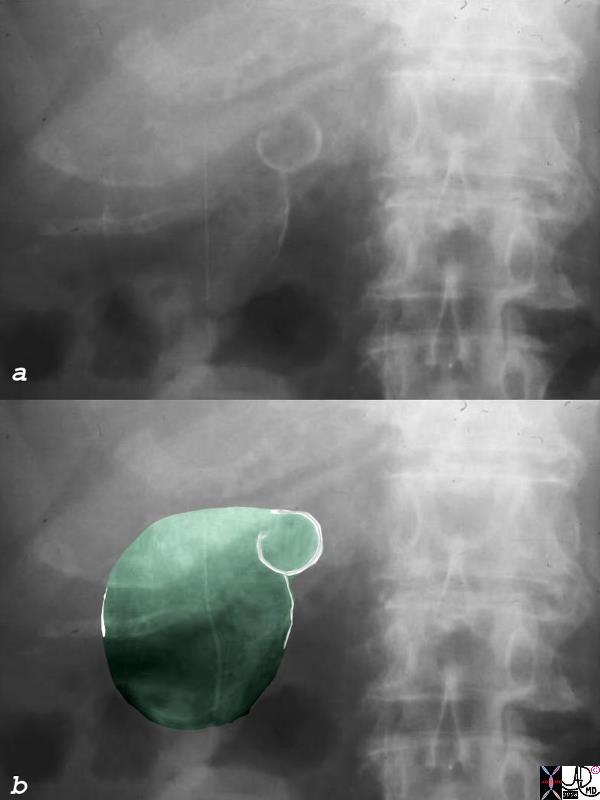
The plain film of the right upper quadrant shows faint calcification (white lines in b)) of the wall of the body and of the entire neck. This finding is subtle since it is intermingled with calcification of the costal cartilage, but it is important and poentially life saving since the patient has to undergo elective cholecystectomy because of the high association with carcinoma. (up to 25% incidence) 04500c01 porcelain gallbladder premalignant plain film plain X-ray calcification calcified wall Courtesy Ashley Davidoff MD copyright 2008 |
|
Porcelain Gallbladder |
|
The gallbladder in this instance is contracted, and has porcelain like calcification. This suggests chronic cholecytitis though no stones are identified. The patient requires to undergo elective cholecystectomy. 47683c01 gallbladder fx calcification in wall calcified wall dx porcelain gallbladder CTscan Davidoff MD |

Porcelain Gallbladder with Calcified Stone |
|
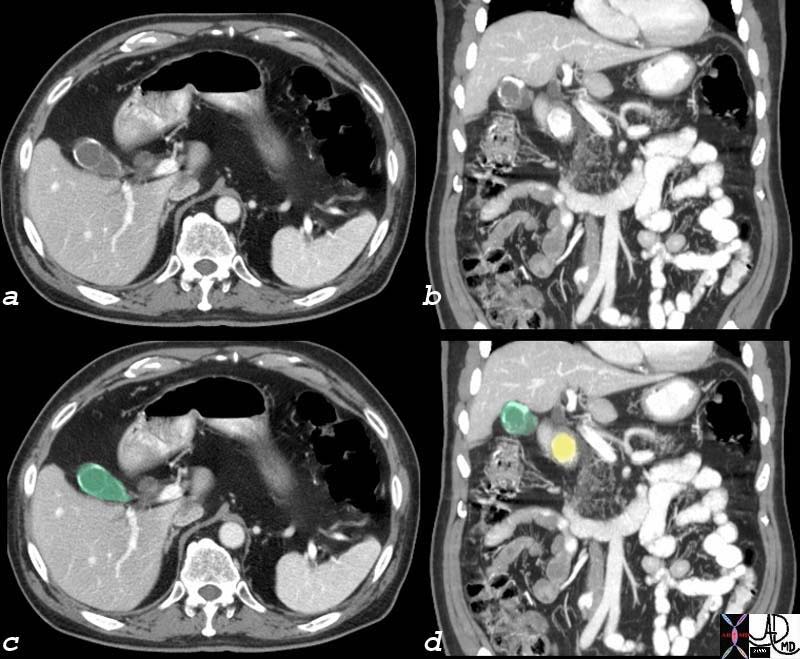
In this CTscan calcification of the wall of the gallbladder (green) is associated with a large calcified stone (yellow) that appears to be impacted in the neck. Cholesterol stones are usually isodense with the bile but in this case it has calcified. The large size of the stone suggests its cholesterol nature in this case. 76225c01 gallbladder wall calcification calcified porcelain gallbladder premalignant CTscan Courtesy Ashley Davidoff MD |

Carcinoma in Situ |
|
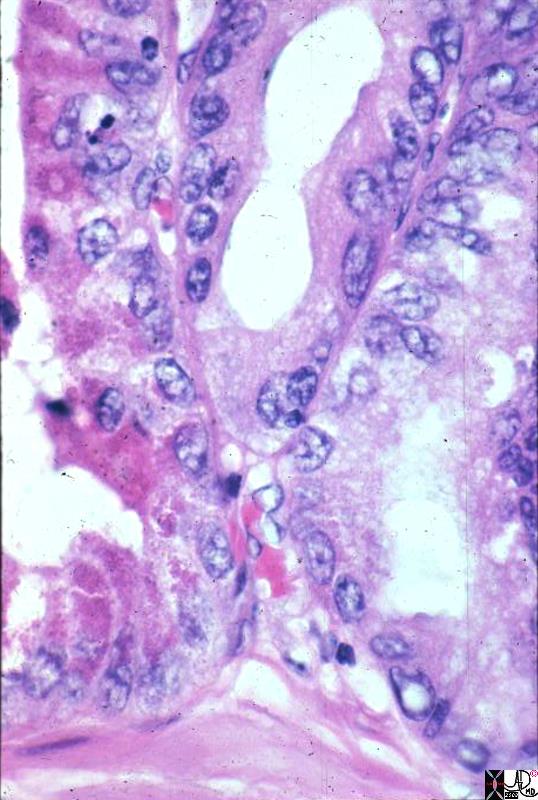
This high power photomicrograph shows the mucosal epithelium and lamina propria, and part of the muscle layer of a gallbladder containing a carcinoma. In this picture, the epithelium is a normal simple, columnar epithelium at one side, (right) and it undergoes a change to a dense, disorganized, malignant epithelium (carcinoma-in-situ) as you follow it across to the other side of the picture. (left) 11946.8s gallbladder carcinoma histopathology Courtesy Barbara Banner MD |
Carcinoma Pleomorphic Nuclii |
|
This medium power photomicrograph shows the epithelium in a case of gallbladder carcinoma. The cells retain a columnar structure, but their nuclei are pleomorphic, and there is variable staining quality of their cytoplasm from cell to cell. Some of the cells look like Paneth cells, with their large, eosinophilic cytoplasmic granules. Variability in size, shape, and staining quality of cells is one of the hallmarks of malignancy. 11943.8s gallbladder carcinoma histopathology Courtesy Barbara Banner MD |
Carcinoma – Back to Back Gland Arrangement |
|
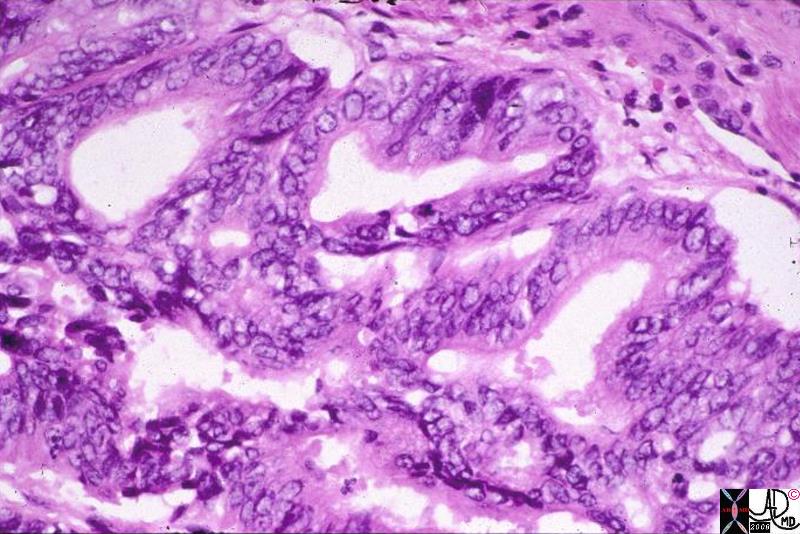
This medium power photomicrograph shows an infiltrating adenocarcinoma of the gallbladder. Note the “back-to-back” gland arrangement, and the irregular distribution of cell nuclei within the glands. The histologic features of this adenocarcinoma are common to adenocarcinomas from many sites, such as the GI tract, pancreas, lung, endometrium etc. but they are also quite typical of gallbladder carcinomas. 11944.8s gallbladder carcinoma histopathology Courtesy Barbara Banner MD |
Carcinoma – Back to Back Gland Arrangement and Irregular Nuclii |
|
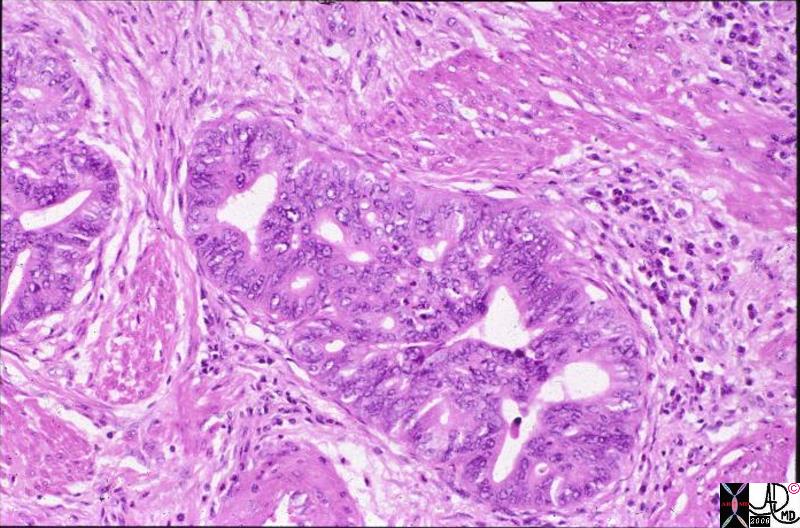
This medium power photomicrograph shows an infiltrating adenocarcinoma of the gallbladder. Note the “back-to-back” gland arrangement, and the irregular distribution of cell nuclei within the glands. The histologic features of this adenocarcinoma are common to adenocarcinomas from many sites, such as the GI tract, pancreas, lung, endometrium etc. but they are also quite typical of gallbladder carcinomas. In this picture the nest of malignant glands is growing across bundles of muscle in the gallbladder wall. The muscle bundles are the deeply eosinophilic structures on either side of the tumor. gallbladder carcinoma histopathology Courtesy Barbara Banner MD 11948s |
Carcinoma – Papillary Form |
|
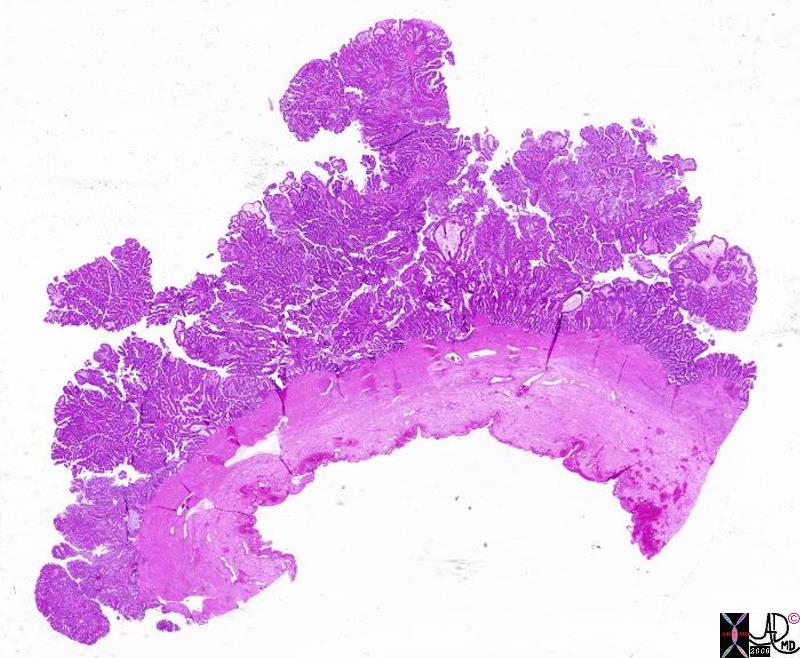
This is a whole-mount section through the wall of a gallbladder with a non-invasive papillary carcinoma. Note how the tumor grows as complex papillary projections, which in the complete specimen projected into and filled up the lumen of the gallbladder. Although this carcinoma is also capable of invading into the wall, this one grew over the interior surface of the gallbladder without invading into the wall. In this picture, the wall is the dense eosinophilic part beneath the papillary projections of the tumor. 11945.8s gallbladder carcinoma histopathology Courtesy Barbara Banner MD |
In the exophytic patterin illustrated above, the neoplasm remains within the wall, taking on a characteristic cauliflower like appearance. The luminal portion can be necrotic, hemmorrhagic and ulcerated.
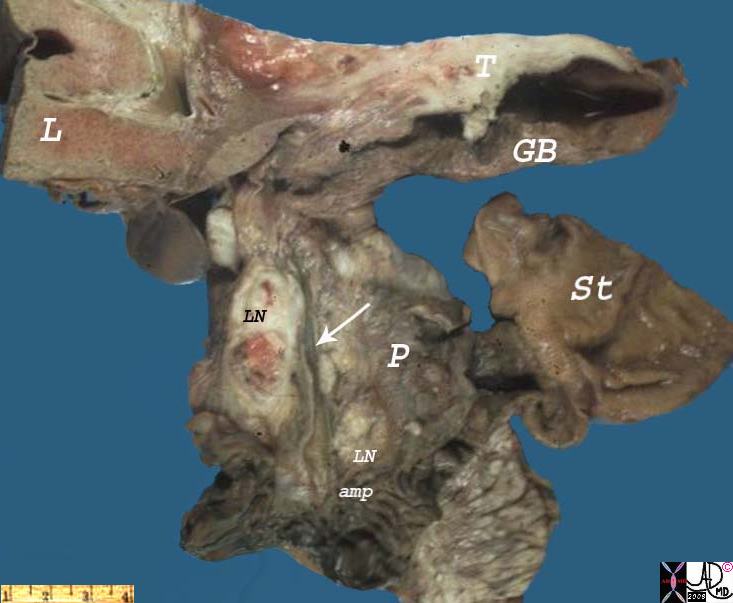
Carcinoma – Lymph Nodes |
|
This picture illustrates the major routes of spread of carcinoma (T) of the gallbladder, (GB) which are direct invasion into the liver, (L) and metastasis to regional lymph nodes. (LN) This is a slice taken through the gallbladder and porta hepatis, including small portions of the liver, stomach, and pancreas, from the autopsy of a patient who died of metastatic carcinoma of the gallbladder. The gallbladder wall is thickened by pale tan-white tumor. (T) The same tan-white tumor is present in lymph nodes (LN – black) of the porta hepatis (cystic node) situated along the common bile duct. These lymph nodes can cause extrahepatic biliary obstruction by compressing the common bile duct as they enlarge. The portions of Ampulla of Vater, (amp) stomach (ST) and pancreas seen in this picture are negative for tumor. Not shown is the fact that this tumor invaded directly through the gallbladder wall and directly into the liver. 11949bs gallbadder carcinoma grosspathology Courtesy Barbara Banner MD |
Carcinoma – Restricted to the Gallbladder
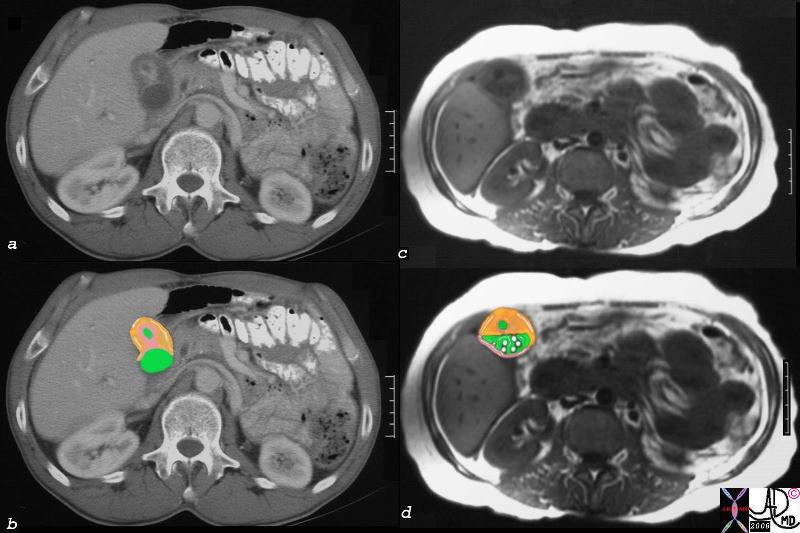
Carcinoma of the Fundus CT and MRI Mucosal and Submucosal Infiltration |
|
In this patient the CTscan (a,b)shows a thick walled and contracted fundus of the gallbladder. The mucosa (pink) and the lamina propria muscular and serosal layer orange are thickened. The fundal lumen is small while the lumen of the body (green) of the gallbladder is normal. This non specific thickening was carcinoma of the gallbladder. The T1 weighted MRI reveals multiple small filling defects in the body of the gallbladder, that were obviously not calcified by CT. By these imaging techniques the carcinoma is confined to the gallbladder (at least macroscopically) and a chance of surgical cure is possible. 16228c03.8s gallbladder wall submucosal tumor = orange mucosal tumor = pink lumen = green thickened mucosa and submucosa carcinoma of the gallbladder CTscan Courtesy Ashley DAvidoff MD copyright 2008 |
Carcinoma – Extending into the Liver via the Gallbladder Fossa
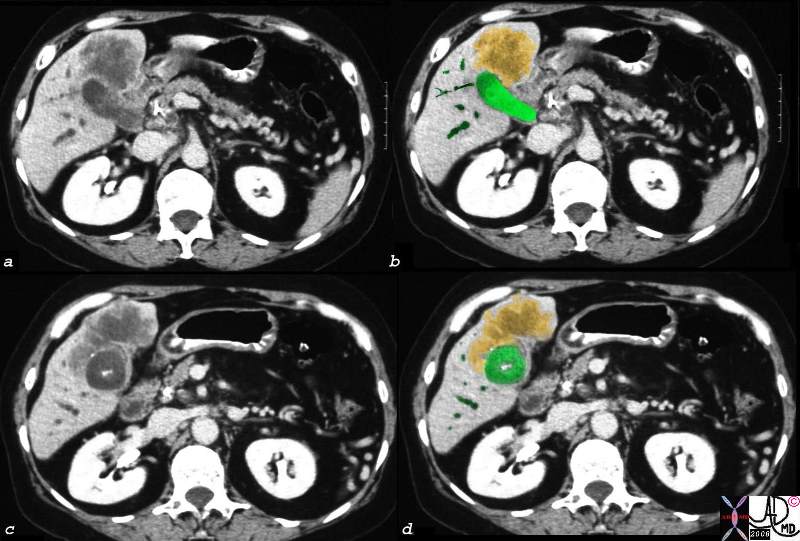
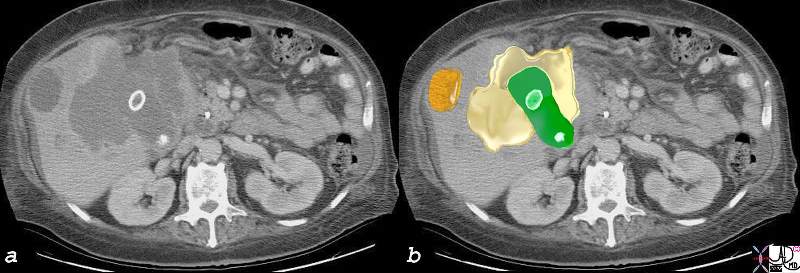
Direct Invasion into the Liver and Bile Duct Obstruction |
|
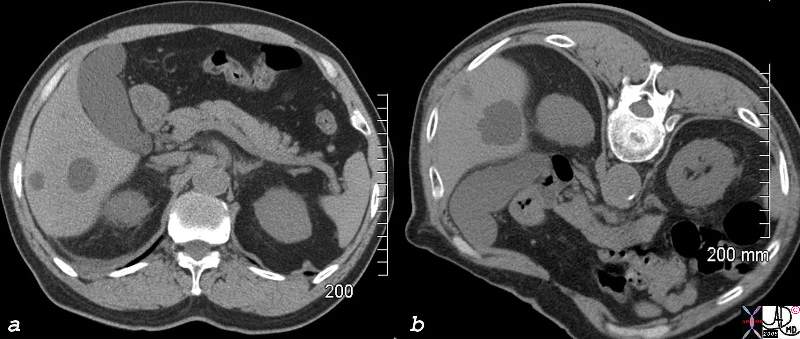
The CTscan of this patient shows a normal sized gallbladder (green) associated with a 4-5cms mass (orange) adjacent to the gallbladder, and extending from the gallbladder fossa. There is asssociated biliary obstruction (dark green tubes) This case represents invasive gallbladder carcinoma with bile duct obstruction. Images c and d show the almost universal association of gallstones in patients with carcinoma. In this case the stones (white) are in the centre of the gallbladder. (green) 16254c03.8s gallbladder anterior wall liver invasion space occupatopn obstruction bile ducts aggressive gallbladder carcinoma complicated by direct invasion metastasis liver windows narroe windws tumor settings gallbladder fossa GBF CTscan Courtesy Ashley Davidoff copyright 2008 |
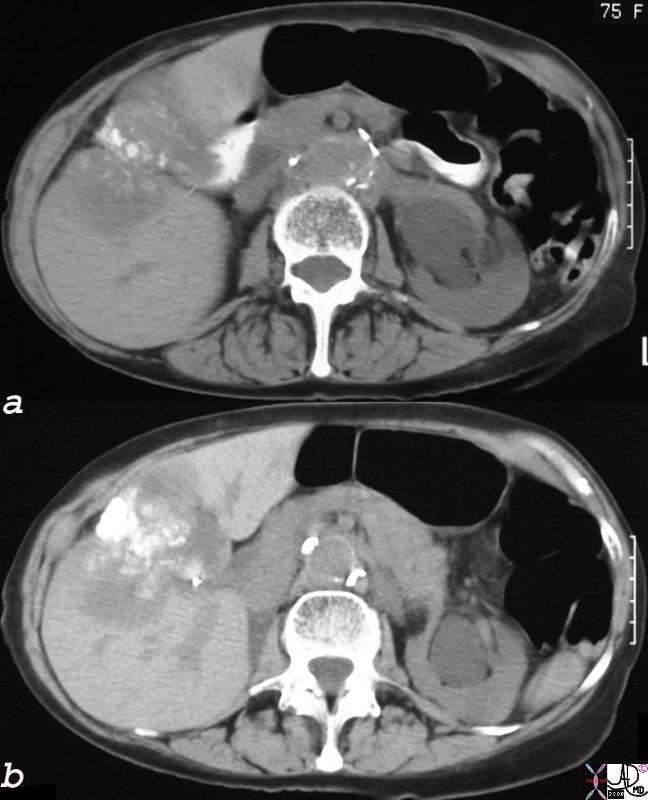
Dystrophic Calcification – Carcinoma of the Gallbladder Extending into the Gallbladder Fossa |
|
The non-contrast CT of the 75year old female patient, shows dystrophic calcification in a mass that seems to be part of the wall of the gallbladder. The mass extends into the liver. These findings are consistent with an inoperable gallbladder mucinous adenocarcinoma, metastatic to the liver by direct extension. Calcification of adenocarcinomas is usually found in the mucinous variant of the disease. 24404c.8s 75 female gallbladder calcification adjacent mass in the liver local invasion into the gallbladder fossa dystrophic calcification probably mucinous adenocarcinoma of the gallbladder carcinoma stones cholelithiasis hydronephrosis |
Carcinoma – Extending into the Liver via the Gallbladder Fossa and Additional Metastases
Local Invasion and Separate Liver Mestastasis |
|
The CTscan in this patient shows two calcified gallstones in the gallbladder (green), with a mass like malignant abnormality extending into the liver on either side (yellow) and a remote metastasis (orange) which is deforming the liver edge. 17280c02b01.8s gallbladder liver mass local invasion cholelithiasis metastasis carcinoma primary gallbladder gallbladder fossa Courtesy Ashley Davidoff MD copyright 2008 |
Disease Extension Beyond the Liver
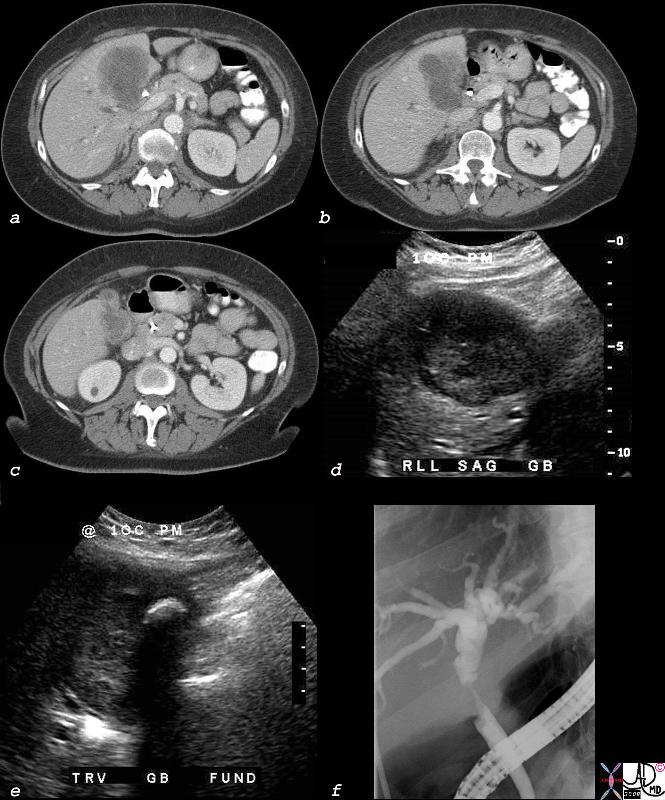
Cholangiocarcinoma with Involvement of the Gallbladder and Bile Duct |
|
The multiple imaging modalities of this patient who is elderly female who presents with obstructive jaundice. Deformity of the gallbladder by CT is noted, with extension of a mass into the surrounding liver (a,b,c) In addition to a mass in the gallbladder (d), the ultrasound shows a shadowing stone (e). An ERCP (f), shows a circumferential stricture of the bile duct. The stricture is in the region of the cystic duct – bile duct junction, with non visualization of the cystic duct suggesting extension of the gallbladder cancer into the cystic duct and bile duct. Lymph node involvement with bile duct obstruction is a less likely possibility due to the circumferential nature of the stricture. 40018c02b.8s elderly female cholelithiasis obstructive jaundice common bile duct stricture dilated intrahepatic ducts irregular enhancing thickening of the gallbladder wall stent gallbladder carcinoma with extension into the CBD or CBD carcinoma with extension into the wall of the gallbladder CTscan USscan ultrasound ERCP Courtesy Ashley DAvidoff MD copyright 2008 |
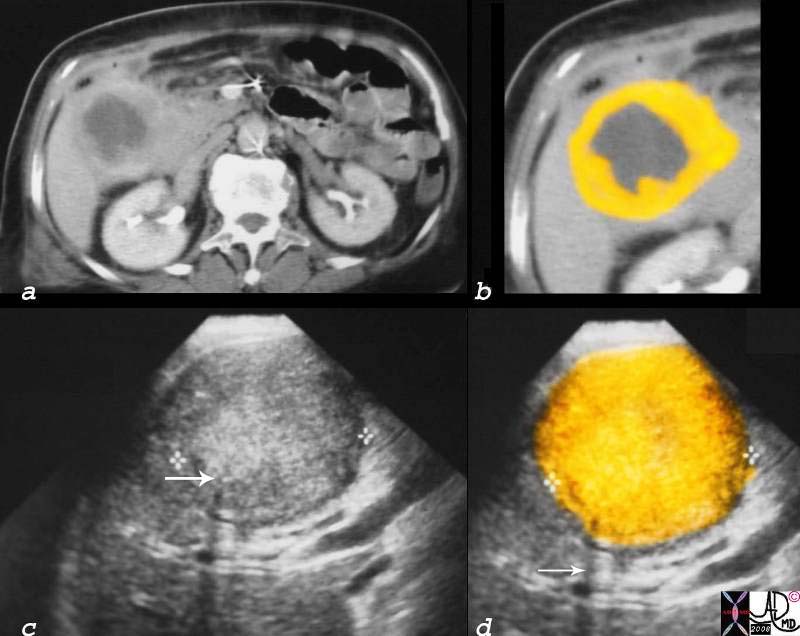
Luminal Invasion |
|
The CT scan through the gallbladder shows a central low density mass (gray) with a surrounding irregular wall (yellow). The ultrasound (c,d), shows complex echoes in the lumen (orange in d) probaly representing a combination of solid mass and tumefactive bile. A single shadowing stone can be seen in c (arrow) with shadowing confirming its presence. (arrow in d) 16254c05 gallbladder space occupation gallbladder carcinoma by CT it appears as a low density centrally and enhancing soft tissue peripherally by USscan looks like the whole lumen is filled with soft tissue tumor question of delayed tumor enhancement vs necrosis CTscan USscan ultrasound Courtesy Ashley Davidoff copyright 2008 |
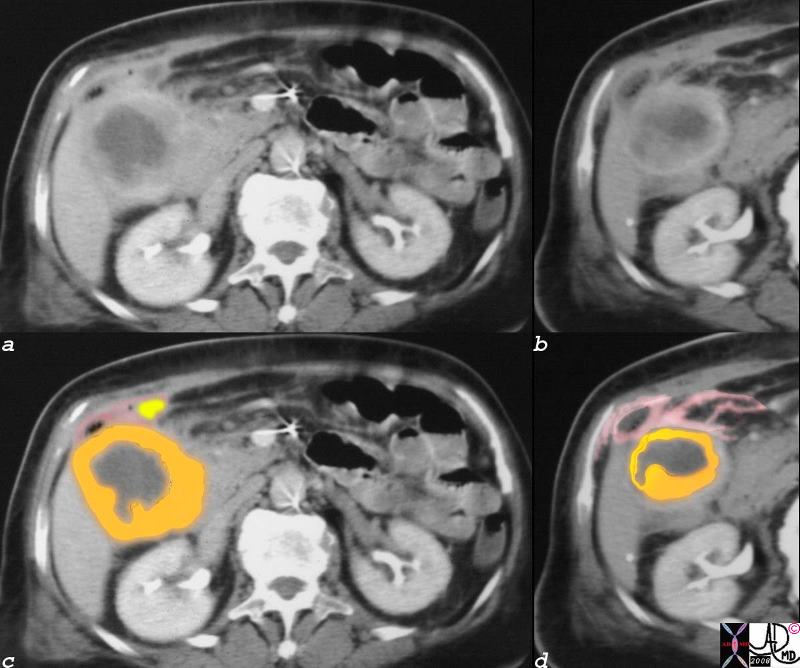
Gallbladder Carcinoma with Perforation and Abscess Formation |
| This is the same case noted above, but it exemplifies extension of the tumor into the surrounding organs, and in this case probably colon with secondary abscess formation (small black airbubbles in c and d ) fluid collection (yellow) in c, and edematous changes in the surrounding fat and peritoneum (pink in c and d). The tumor has central non enhancing matrix (gray) surrounded by more solid enhancing tumor (orange)
16254c01b02.8s gallbladder thickened irregular wall air anterior wall small fluid collection gallbladder carcinoma complicated by perforation and abscess formation CTscan Courtesy Ashley Davidoff copyright 2008 |
Conclusion
From the anatomical point of view it is interesting to note that gallbladder cancer occurs most commonly in the fundus, and from the pathophysiological point of view it is so frequently associated with gallstones. It is attractive to consider the fact that in the “day” position of the gallbladder, the most dependant, concentrated bile is in contact with the mucosa, and similalrly stones will be in contact with the fundal mucosa for the longest time. In the prone position (if the person sleeps in prone position) stones will be in contact with the anteriorly positioned fundus as well. hence chronoic contact, chronic irritation of the fundus and aberrant chemical environments such as excessive bile salts, or cholesterol make a fertile environment for the evolution of the mucosa to dysplasia and carcinoma.
 Gallbladder Cancer and Stones Gallbladder Cancer and Stones |
| The greenpepper sectioned in long axis has a mass like base, and remnant seeds reminiscent of the combination of fundal carcinoma in the presence of cholelithiasis.
11528b.8 gallbladder food in the body green pepper cancer carcinoma gall stones cholelithiasis Davidoff art Davidoff photography copyright |
References
Denshaw-Burke Mary Denshaw-Burke, MD, Gallbladder Cancer eMedicine 2008
Szarnecki Gregory M Szarnecki, MD, Gallbladder, Carcinoma e Medicine 2007
References provided by e Medicine
National Cancer Institute. Treatment statement for health professionals: gallbladder cancer. Updated 2/15/07. Med News. Available at http://www.meb.uni-bonn.de/cancer.gov/CDR0000062904.html. Accessed August 23, 2007.
Fong Y, Wagman L, Gonen M, et al. Evidence-based gallbladder cancer staging: changing cancer staging by analysis of data from the National Cancer Database. Ann Surg. Jun 2006;243(6):767-71; discussion 771-4. [Medline]. [Full Text].
Levy AD, Murakata LA, Rohrmann CA Jr. Gallbladder carcinoma: radiologic-pathologic correlation. Radiographics. Mar-Apr 2001;21(2):295-314; questionnaire, 549-55. [Medline]. [Full Text].
Douglass HO Jr, Kim SY, Merpol NJ. Neoplasms of the gallbladder. In: Holland JF, Frei E III, Best RC Jr, eds. Cancer Medicine. Vol 2. 4th ed. Baltimore, Md: Williams & Wilkins; 1997:1955-63.
Dudiak CM, Lawson TL. Carcinoma of the gallbladder. Diagnostic Ultrasound (Second Series) Test and Syllabus. St Louis, Mo: Mosby-Year Book; 1994:324-62.
Elsayes KM, Oliveira EP, Narra VR, El-Merhi FM, Brown JJ. Magnetic resonance imaging of the gallbladder: spectrum of abnormalities. Acta Radiol. Jun 2007;48(5):476-82. [Medline].
Grainger RG, Allison E. Grainger and Allison’s Diagnostic Radiology: a Textbook of Medical Imaging. Vol 2. 3rd ed. New York, NY: Churchill Livingstone; 1996:1224.
Greene FL, Page DL, Fleming ID, eds. Gallbladder. AJCC Cancer Staging Manual. 6th ed. New York, NY: Springer-Verlag; 2002:139-44.
Haubrich WS, Schaffner F, Berk JE, eds. Bockus Gastroenterology. Vol 3. 5th ed. Philadelphia, Pa: WB Saunders; 1995:2739-44.
Kai M, Chijiiwa K, Ohuchida J, et al. A curative resection improves the postoperative survival rate even in patients with advanced gallbladder carcinoma. J Gastrointest Surg. Aug 2007;11(8):1025-32. [Medline].
Kim MJ, Kim KW, Kim HC, et al. Unusual malignant tumors of the gallbladder. AJR Am J Roentgenol. Aug 2006;187(2):473-80. [Medline]. [Full Text].
Mekeel KL, Hemming AW. Surgical management of gallbladder carcinoma: a review. J Gastrointest Surg. Sep 2007;11(9):1188-93. [Medline].
Memel DS, Balfe DM, Semelka RC. The biliary tract. In: Lee JKT, Sagel SS, Stanley RJ, eds. Computed Body Tomography With MRI Correlation. Vol 2. 3rd ed. Philadelphia, Pa: Lippincott-Raven; 1997:810-3.
Miller G, Schwartz LH, D’Angelica M. The use of imaging in the diagnosis and staging of hepatobiliary malignancies. Surg Oncol Clin N Am. Apr 2007;16(2):343-68. [Medline].
Numata K, Oka H, Morimoto M, et al. Differential diagnosis of gallbladder diseases with contrast-enhanced harmonic gray scale ultrasonography. J Ultrasound Med. Jun 2007;26(6):763-74. [Medline].
Oe A, Kawabe J, Torii K, et al. Distinguishing benign from malignant gallbladder wall thickening using FDG-PET. Ann Nucl Med. Dec 2006;20(10):699-703. [Medline].
Shih SP, Schulick RD, Cameron JL, et al. Gallbladder cancer: the role of laparoscopy and radical resection. Ann Surg. Jun 2007;245(6):893-901. [Medline].
Srivastava AK, Singh B, Gupta SL. Prevalence of Toxoplasma antibodies in sheep and goats in India. Trop Anim Health Prod. Nov 1983;15(4):207-8. [Medline].
Vitetta L, Sali A, Little P, Mrazek L. Gallstones and gall bladder carcinoma. Aust N Z J Surg. Sep 2000;70(9):667-73. [Medline].
Yamada T, Alpers DH, Owyang C, Powell DW, Silverstein FE, eds. Textbook of Gastroenterology. Vol 2. 2nd ed. Baltimore, Md: Lippincott Williams & Wilkins; 1999:2335-40.