
Clinical Considerations in Gallbladder Disease
Copyright 2008
Clinical Diagnosis
Diagnosis is a determination of the nature of a disease. An orderly and progressive diagnostic algorithm must be followed in order to arrive at the most accurate diagnosis, in order to institute the most effective treatment. The meticulous attention to the nature of the pain and its associated symptoms in the clinical history, a focused examination, followed by relevant laboratory investigation and by appropriate diagnostic imaging is necessary. Of these, the most important is the clinical history.
Medicine – Research Teaching and Clinical Care |
| 85331p.800 people white coats medicine laboratory group discussion conversation education clinical management white coats students scholars teacher physician student relationship Courtesy Edward Smith MD |
History Taking – Symptoms -Pain
As we have seen from the previous modules, pain is complex and often individualized. The most common complaint of gallbladder disease is pain, usually right upper quadrant pain. Gallbladder pain is usually caused as a result of a stone passing into the biliary ducts and causing biliary colic or as a result of a stone obstructing the gallbladder if it is impacted in the neck of the gallbladder or the cystic duct. Gallbladder pain is usually acute and initially tends to be of visceral in origin as the gallbladder becomes distended. It is initially aching and ill defined. If inflammation or infection ensues then the pain spreads to the peritoneal lining and it becomes somatic in nature, and by definition a little sharper and better localized.
Pain Descriptors
Pain descriptors are verbal terms used to characterize pain. Although they are subjective expressions of pain, descriptors can be organized into helpful tools when assessing a patient. The purpose of using pain descriptors is two fold: First, they provide structure to an otherwise subjective interview. Secondly they may remind the atient of aspects of the pain thaey might not have volunteered or remembered.
Although physical diagnosis texts vary, the most common descriptors include preciptating factors, duration, onset, character, situation, severity, aggravating and relieving influences, radiation and associated symptoms. The acronym is PDOCSSARRA. Other descriptors like pattern, location and level of impairment may be added to bring more depth to the patient’s story, keeping in mind the time constraints of the healthcare setting.
About 70 percent of patients who experience pain related to the gallbladder or bile duct have had similr experience before andthey ascribe the pain to “my gallbladder pain”.
Precipitating factors
“What were you doing when the pain started?” The most classical description usually noted by clinicians is that the gallbladder colic is often precipitated by eating a fatty meal, (pizza, cheese, or fried meal) which causes the gallbladder to contract and potentially push a small stone into the neck or cystic duct precipitating acute gallbladder colic. Sometimes the stone will pass the cystic duct and go into the bile duct precipitating biliary colic. Thus the presentation may take a few forms – gallbladder colic and biliary colic and they are different in their clinical manifestations. When complications such as acute cholecystitis or cholangitis evolve, then the pain suyndromes and clinical manifestations change.
Duration
Time and pain can be framed in two important of contexts. The first is its historical context “How long have you had the pain for?” , and the second is “How long does the pain last?”
The pain starts out gradually presumably due to early distension of the gallbladder, becoming more intense. Sometimes the intensity becomes more severe over a 1-2 hour period sometimes up to 5 hoours, but on occasion it may take several days and even up to a week. It is presumed that inflammatory changes and or infection precipitate the acceleration of pain as somatic structures and innflammatoion reduces thresholds, causing the pain to localize and become more severe.
The second question of “How long does it last?” also has significant relevance gallbladder colic can last from 30 minutes to up to 3-4 days, but usually 2-3 hours. Gallbladder disease is a s a result of cholelithiasis. If stones are passed through the cystic duct and get caught in the bile duct they can cause biliary colic which is usually less severe since somatic nociceptors are not affected. It also is shorter lasting, in the 2-3 hour range since the stones commonly pass.
Onset
“Did it start suddenly or slowly?” or “Did it build up quickly to peak or slowly to peak?” are the type of questions that define onset. In general pain that starts suddenly, is somatic in origin while pain that is gradual in origin is usually visceral. Thus “onset” describes the arrival of pain.
The pain usually starts out as a mild becoming gradual and steady.and vague discomfort as the gallbladder begins to distended.
Character
“What did it feel like? We are now getting to the exciting part of the story. Was it sharp, cutting, pinching shooting, stabbing, knife like or dull and bruise like? Was it throbbing, gripping aching, tearing, lancinating or like lightning. Did it feel like pressure, heaviness, dull or nauseating or more like real piercing pain? What is colicky, spasmodic or squeezing like bad gas cramps?” Was it tingling or numb like.
The pain of acute cholecystitis starts out as mild, ill defined and ache like. Even though it may be called “colic”, it is in fact more constant rather than a pain that comes in colicky waves. If the stone falls back into the gallbladder or passes then the pain abats. If the stone becomes impacted, the disease evolves and the pain becomes more intense, unremitting, and unbearable. Edema and spasm may cause urther narrowing and causing more severe impaction. Pain at this stage is unabating.
Situation
” Where exactly does it hurt? Can you point with a finger or is it easier to use your hold hand to define the position of the pain?” “Does it feel deep or does it feel like it is coming from the muscles or skin?”
Also called location, situation defines the affected area of the body and the depth of pain as either superficial or deep. The situation can vary from well localized pain to that which is perceived to originate from a general area that is not well defined.
In acute cholecystitis it is located in the right upper quadrant or epigastrium of the abdomen, initially diffuse and deep, but if the peritoneum is involved then somatic type pain surfaces as peritonism. Somatic pain tends to be well localized in which case the patient points with a finger, while visceral pain tends to be more diffuse and the patient uses the whole hand to decribe the location of the pain.
Severity
“How severe is the pain?” “Is it the worst pain of your life or is only mild?” On a scale of 1-10 with 1 being mild and 10 being the worst ,where does it fit into the scale?”
With the question of severity we start to get into individual perception of pain. What may be severe pain for one person may be mild for another. There have been several classifications used to evaluate the severity of pain.
Patients sometimes describe gallbladder pain as worst pain the patient may have suffered, though when the stone spontaneously dislodges, then it may be short lived and mild.
Aggravating Factors
“What makes the pain worse?”
In general while the pain is visceral it is constant, gradually becoming worse with no relieving features. When the peritoneal surface becomes involved touching the area and on occasion deep inspiration may aggravate the pain.
Relieving Factors
“What makes the pain better?” “Does anything help the pain?” “What medicine have you taken, and has it been effective?”
In general as long as the stone is impacted nothing short of strong analgesics are helpful.
Radiation
“Does the pain radiate anywhere else in the body?”
Gallbladder pain may radiate to the back or infrascapular region. On occasion it can radiate to the left upper quadrant.
Associated Symptoms
“What other symptoms do you have with the pain?” “Are you nauseous?” Did you vomit? Did you sweat? “Did you faint?” Did you have diarrhea?” “Did somebody comment that you were pale?” Were you short of breath?
As the distension of the gallbladder or biliary system advance, autonomic involvement with nausea and vomitting may be a consequence.
Clinical Examination- Signs
Clinical signs are limited in entities that involve the gallbladder.
Jaundice
Biliary stones with obstruction (choledocholithiasis) may be present with jaundice. This is relatively uncommon.
Murphy’s sign
In the case of biliary or gallbladder colic, or in patients with suspected choelcystitis, it is important to attempt to elicit Murphy’s sign. The examining hand is gently placed on the patient’s right upper quadrant, in the mid clavicular line at the about the level of the 9th rib. Deep palpation is slowly advance to about 1-2 inches deep, and the patient is asked to take a deep breath. In the presence of an inflammed and distended gallbladder there will be a sudden cessation of inspiration due to pain caused by the gallbladder moving forward onto the palpating hand. Sometimes, if focal peritonitis is present the pain is present even with light or mild compression in the RUQ.
Courvoisier’s sign
The other sign that is important to know about is Courvoisier’s sign which is a non painful palbable gallbladder in the presence of painless jaundice. This infers pancreatic cancer which has caused obstruction of the the distal common bile duct as well as slowly progressive distension of the the gallbladder (hence painless).
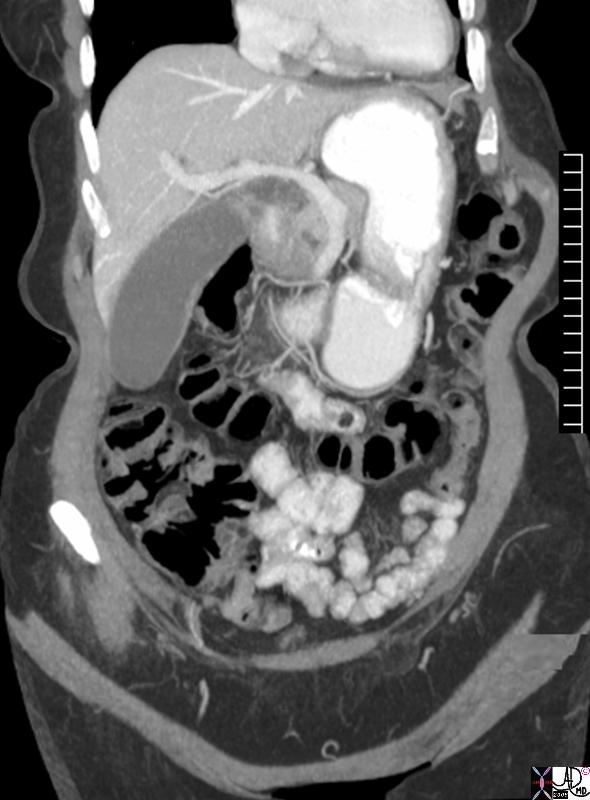
Position of the Gallbladder
Mid Clavicular Line – 9th Rib
The first diagram is from the work of da Vinci and the gallbladder is ringed in red. Its classical surface anatomy positions it in the midclavicular line medial to the 9th rib. The second image is a coronally reconstructed CTscan shows an asymptomatic, zucchini shaped elongated gallbladder that is positioned in the right upper quadrant. 76764.8s elderly femal gallbladder elongated sausage shape zuchini shape transverse dimension 4.5 cms longitudinal dimension 12.5cms aging gallbladder vs enlarged? CTscan Courtesy Ashley DAvidoff MD copyright 2008


Abdominal Pain – Midgut |
| 22779 hand abdomen clinical periumbilical pain midgut pain scout KUB CTscout Courtesy Ashley Davidoff MD |
LAb Studies
Usually not helpful but there may be a leukocytosis and bandemia