
Copyright 2008
Alok Anand
Definition
HIV cholangiopathy, or more appropriately AIDS associated Cholangiopathy is a group of clinical findings caused by opportunistic infections of the biliary system in the immunocompromised patient.
Structurally it it is characterized by strictures and atrophy of the biliary tract, usually in sub-hepatic segments. It manifests with periportal adenopathy, hepatomegaly, and acalculous cholecystitis, sclerosing cholangitis, papillary stenosis, or cholelithiasis. In some cases pancreatitis may be present. This may also be associated with Kaposi’s sarcoma, a cancer causing vascular tumors caused by Human Herpes Virus 8, or lymphoma.
Clinically patients may present with anicteric (non-jaundiced) cholestatis and symptoms often include right upper quadrant pain and high fever. On further evaluation patients often have elevated cholestasis markers, and liver enzymes. As is often the case in biliary disease, these features are often non-specific and may resemble the primary forms of biliary disease.
As such, diagnosis relies heavily on clinical suspicion in the presence of an immunocompromised patient, and may be suggested by laboratory tests, blood cultures, and confirmed by imaging. This may be imaged by MRI (MRCP), and ERCP. Of note this disease process was first described by ERCP. Papillary stenosis may be present.
As this is a disease of opportunistic infection, the typical findings are that of fungal, protozoan, or bacterial agents. Patients may also have pre-existing viral heptatis, and would have consequent image findings. The most common agents, however, are cryptosporidium parvum and cytomegalovirus. Typically, in patients with fungal or mycobacterial (TB) infections, granulomatous changes are noted in both the bile ducts, as well as liver parenchyma. Typically symptomatic patients are significanty immunocompromised, with CD4 type T lymphocyte counts of approximately 100/cc.
Some notable imaging patterns include intrahepatic ductal dilatation with beading with strictures within the hepatic biliary tree. More distally, patients will have more focal strictures of the common bile duct with proximal dilatation.
Treatment depends on the cause sometimes being of a surgical nature where dilatation, stent placenet or papillotomy is resquired and sometimes being medical with appropriate anti fungal or antibacterial medication.
Gallbladder fossa |
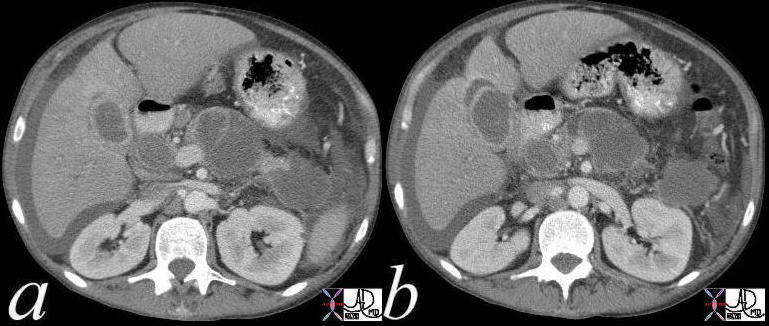
| HIV positive patient with known pancreatitis and a fever 41249c Courtesy Ashley Davidoff MD code pancreas pseudocysts code gallbladder fx fluid in the fossa imaging radiology CTscan inflammation infection(Image courtesy of Ashley Davidoff M.D.) |
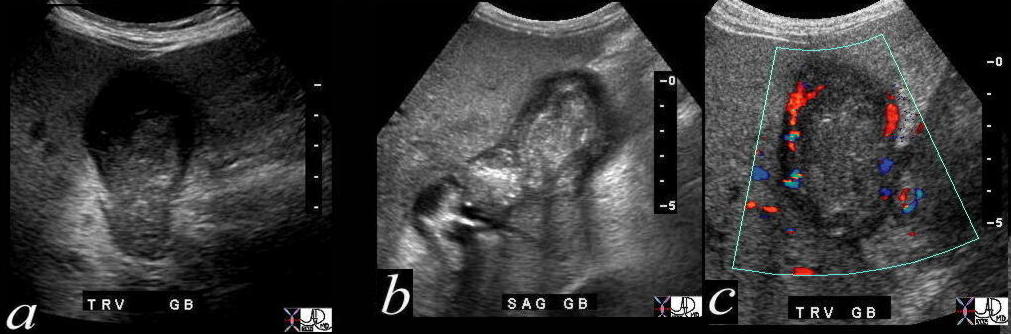
Cholecystitis probably Cryptosporidium |
| 41257c004 Courtesy Ashley Davidoff MD gallbladder filling defect question sludge fx hyperemic wall dx HIV cholangiopathy chronic cholecystitis subacute cholecystitis imaging radiology USscan mechanical inflammation |
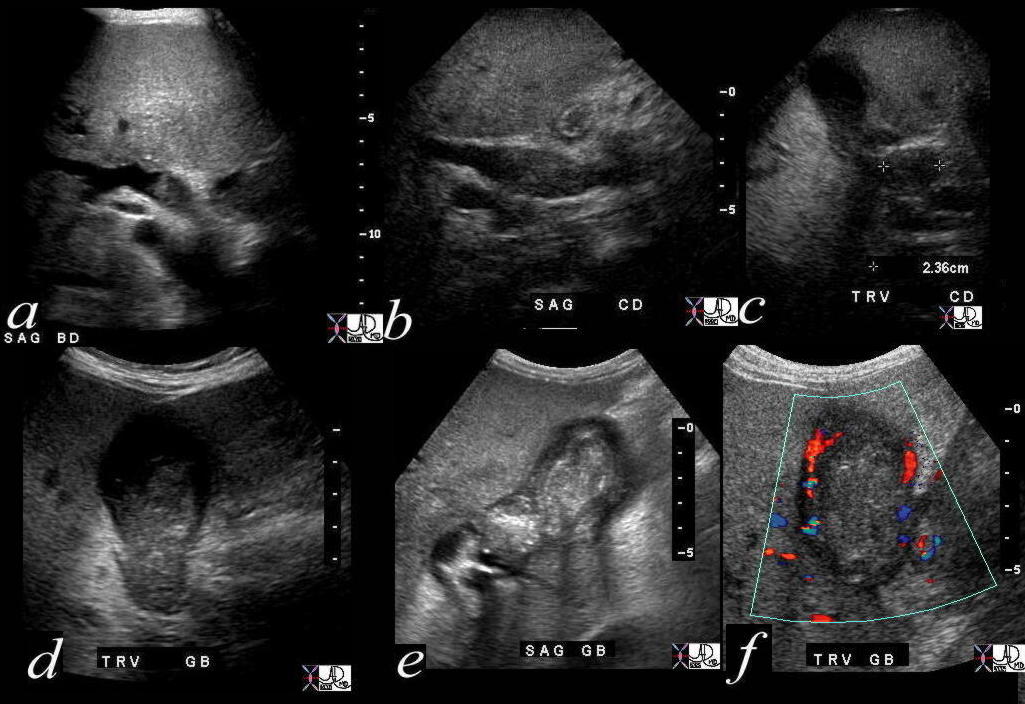
Cholecystitis probably Cryptosporidium |
|
41257c005 Courtesy Ashley Davidoff MD code gallbladder filling defect question sludge fx hyperemic wall bile duct filling defect question sludge fx enlarged dilated dx HIV cholangiopathy chronic cholecystitis subacute cholecystitis imaging radiology USscan mechanical inflammation |
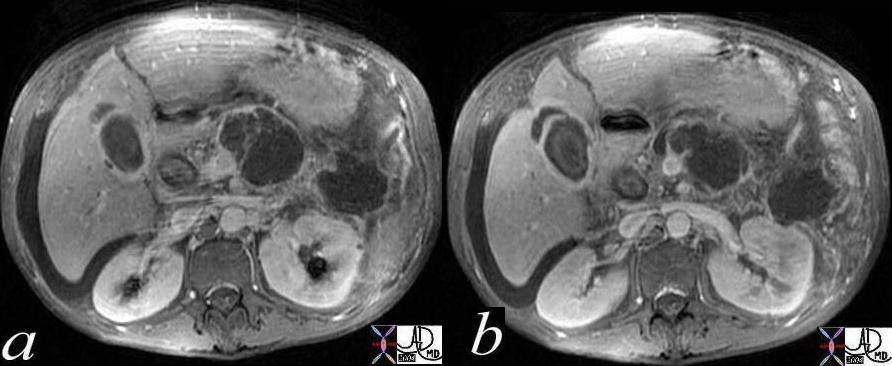
HIV Cholangiopathy |
| 41267c01 Courtesy Ashley Davidoff MD code pancreas pseudocysts code gallbladder fx fluid in the fossa dx HIV cholangiopathy chronic pancreatitis imaging radiology CTscan inflammation infection |