
Introduction
The layers of the gallbladder conform to the basic pattern seen in the histology of other structures in the gastrointestinal tract, except that rather than having 4 layers (mucosa, submucosa, muscularis and serosa/adventitia), it has 3 layers (mucosa , muscularis and serosa/adventitia). There is a distinct absence of a submucosa.
Principles
Basic Histologic Makeup of Gastrointestinal Tract
Basic 4 Layered Structure of GI tract Histologic Layers |
|
This image shows 4 layers of of tissue characteristic of the histology of many gastrointestinal structures. A simple columnar epithelium is the the inner cellular layer of the mucosa, and it is supported by a muscularis mucosa (pink). The submucosa (yellow) consists of loose connective tissue with blood vessels lymphatics and macrophages. The muscularis (red) is next and is followed by the outer covering (white) which may be a serosa or adventitia. The histology of the gallbladder does not conform exactly. It does have a simple columnar epithelium, lacks a muscularis mucsoa, but has a lamina propria as part of the mucosa that houses blood vessels and lymphatics. This layer is followed by an ill defined muscular layer that is intermingled with collagen and elastic tissue, and is covered on its free surface by a serosa and liver surface by an adventitia. 32347 tube colon small bowel lung bronchus bronchi esophagus stomach large bowel bile duct ureter tube principles Courtesy Ashley DAvidoff MD Davidoff art mucosa submucosa muscularis adventitia serosa histology |
Histological Makeup of the Gallbladder Wall
The gallbladder wall has 3 major layers; mucosa muscularis and serosa/adventitia. It lacks a distinct submucosa, but also lacks a muscular layer in the mucosa (muscularis mucosa ). The lamina propria functions as a submucosa to house blood vessels and lymphatics but it is tucked intoo the folds of the gallbladder, and is rapidly within a short distance frrom the fiolds followed by the muscularis layer.
There is also a difference in the wall of the gallbladder that abuts the liver and the wall that abuts the peritoneal cavity.

Whole Mount of the Gallbladder Basic 3 Layered Histological Structure of the Gallbladder |
|
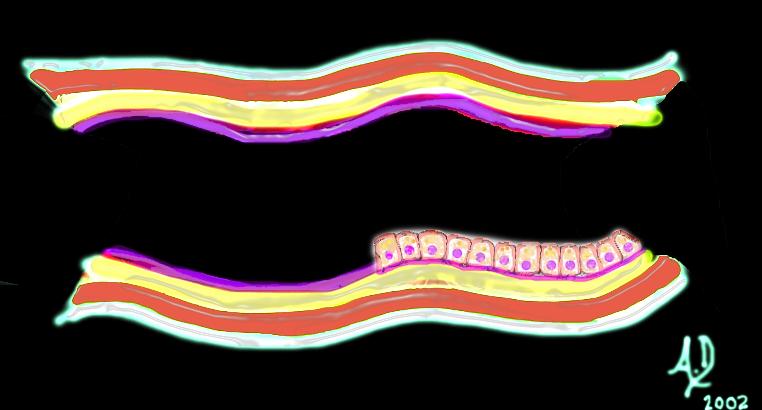
The upper and lower images represent whole mounts of a normal gallbladder. The upper image shows the liver surface of the gallbladder and the region of the gallbladder fossa, the lumen, and the free wall that is covered by the peritoneum. The lower image shows the three basic histological layers. The pink mucosa, the red muscularis, and the white outer serosa. 00139c11s gallbladder histology normal gallbladder fossa free wall peritoneal lining whole mount mucosa histology Courtesy Ashley Davidoff MD copyright 2008 |
Ultrasound examination of the gallbladder is performed in the fasting state and it is therefore distended. When the gallbladder is distended, the three layers cannot be distinguished. When the gallbladder is contracted, three distinct layers representing echogenic mucosa hypoechoic muscularis and echogenic serosa adventitia become obvious.

Three Layers Noted in the Contracted Gallbladder |
| In this ultrasound image of the contracted gallbladder, three distinct layers are obvious. The inner echogenic mucosa abuts the lumen, the hypoechoic muscular middle layer is the thickest, while the outer layer is most echogenic since it contains a relatively large amounts of collagen.
1632H5~1.8s gallbladder wall layers mucosa submucosa muscularis serosa thick walled contracted USscan ultrasound Courtesy Philips Medical Systems copyright 2008 |
Mucosa
The folds of the mucosa that project toward the lumen are frond-like in form and are quite irregular and non uniform when viewed in comparison to the folds of the small bowel for example. The mucosa consists of a tall columnar epithelium with basal nuclii and pale cytoplasm (due to sulfomucins) and lack goblet cells. In the neck however mucus secreting goblet cells are found. The mucosal layer secretes mucous to protect the gall bladder from the relatively alkaline bile it stores. (pH 7.6 -8.6)
Low Power of the Wall of the Gallbladder |
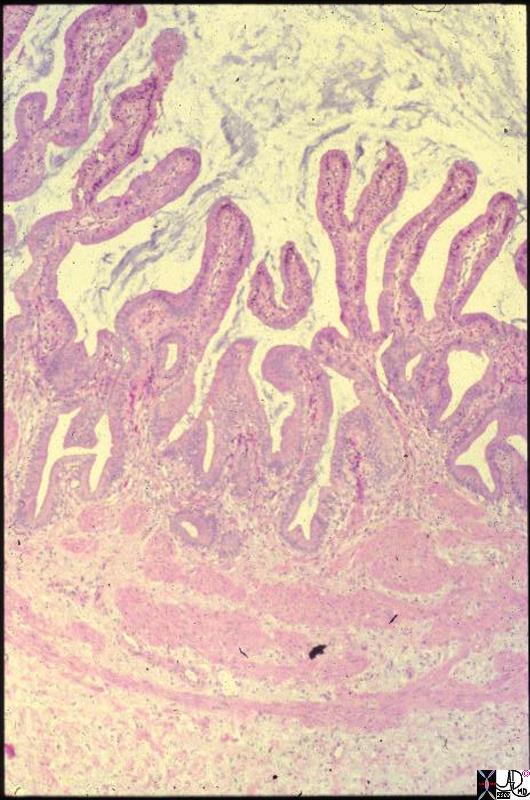
| This is a low power photomicrograph of the wall of a normal gallbladder. Note the delicate finger-like projections (fronds) of the mucosa. The lanina propria (submucosa functional equivalent) is tucked into the folds. Just under the folds is the muscularis mucosa, seen here as loosely connected bundles of smooth muscle. Deep to that is some connective tissue of the gallbladder bed. On its peritoneal aspect the gallbladder is covered only by a single layer of mesothelium. Thus, the gallbladder has a much simpler wall structure than the GI tract. The thickness is only about 2 mm. The implications for penetration of stones, spread of inflammation, and perforation are obvious.
gallbladder histology Courtesy Barbara Banner MD 11905.8s |
Lamina Propria
Deep to the epithelium, the lamina propria contains abundant capillaries and larger blood vessels. The epithelial layer and the lamina propria comprise the mucosa.
Mucosa of the Gallbladder |
|
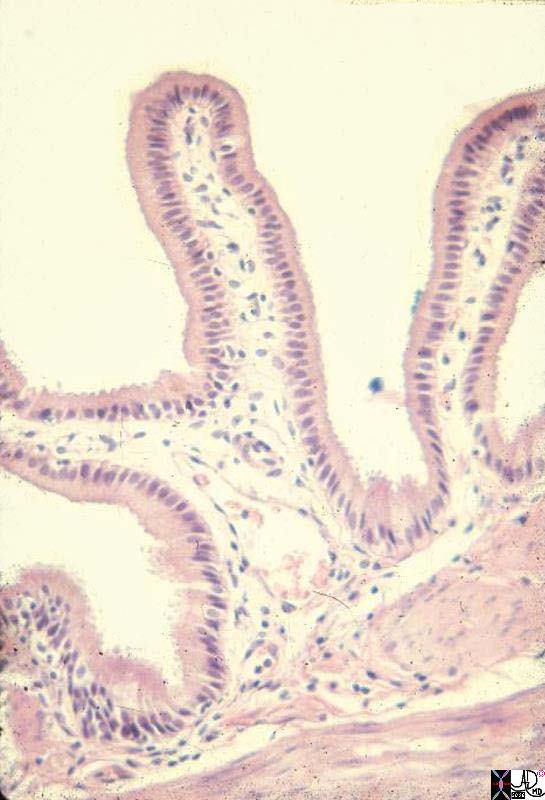
This is a medium power photomicrograph showing how delicate the mucosal fronds are. Each frond consists of a single layer of columnar epithelium covering a core of capillaries and a few fibroblasts. The empty upper part of the image is the gallbladder lumen, and on the opposite lower side, parts of two muscle bundles can be seen. gallbladder histology Courtesy Barbara Banner MD 11906.8s |
Muscularis
Next there is a smooth muscle layer called the muscularis externa appearing as irregular layers of smooth muscle, connective tissue and elastic tissue. The inner components align longitudinally and the outer align diagonally so that they spiral around the gallbladder.
Serosa/Adventitia
The peritoneum covers the gallbladder on its free surface and so in that location a serosa is formed. There is no peritoneum in the gallbladder fossa and so in this region it is called an adventitia.
In 10% of people aberrant vestigial ducts of Luschka project from the liver into the wall of the gallbladder without connecting to the gallbladder lumen. There are also larger accessory ducts that communicate with the cystic or hepatic ducts.
Rokitansky Aschoff Sinuses
The Rokitansky-Aschoff sinuses are diverticula or pockets in the wall of the gallbladder that may be microscopic or macroscopic. They are thought to be an acquired abnormality caused by increased intraluminal pressure resulting in mechanical stresses on a mucosa and outward bulging of the mucosa..
Structurally they are characterized as outpouchings of the gallbladder mucosa into and sometimes extend beyond the gallbladder muscle layer. They are not of themselves considered abnormal, but they seem be associated with elevated pressures in the gallbladder possibly as a result of normal and hypercontractile states and are also associated with chronic cholecystitis and cholelithiasis which may have similar pathogenetic mechanisms.
The diverticula do not cause functional impairment.
No clinical impairment is therefore implicated but they are associated with the hyperplastic cholecystoses (adenomyomatosis and cholesterolosis) as well as gallstone disease. Sometimes calcific concretions accumulate within the diverticulum.
When the diverticula are large the diagnosis is usually accomplished by ultrasound, and less commonly by CT or MRI.
Treatment is only considered when a patient presents with right upper quadrant pain and no other cause can be found. In some patients symptomatic relief has been accomplished with cholecytectomy.
Rokitansky-Aschoff Sinus |
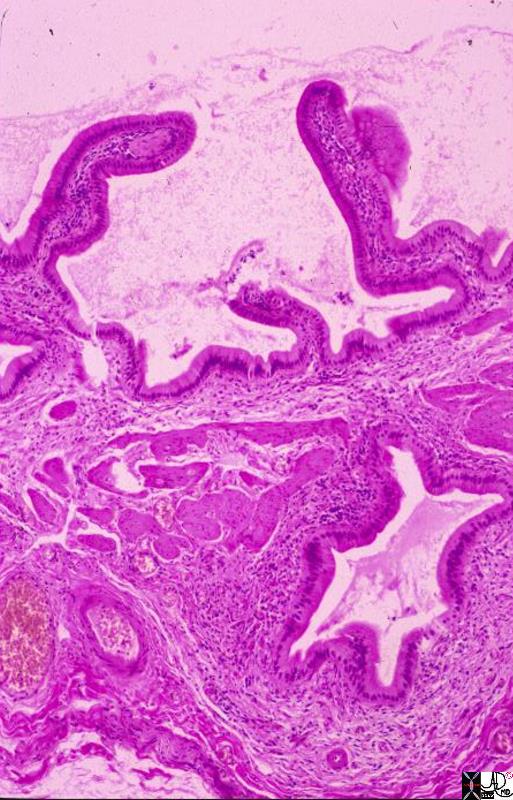
| This is a low power photomicrograph showing full thickness gallbladder wall. The lumen is the empty part with mucosal fronds projecting into it. The prominent hole deep in the wall is a Rokitansky-Aschoff sinus. This one is seen in cross section, but in vivo the sinuses are in continuity with the lumen because they are diverticula, or protrusions of mucosa out through the muscular layer, possibly in response to increased pressure from gallstones. Note that the sinus is lined by a single layer of columnar epithelium, just like the lumen itself. Because they are lumenal projections, these sinuses become filled with bile. Gallstones can become impacted in them. In acute cholecystitis, inflammation can spread directly through the wall following the Rokitansky-Aschoff sinuses. In chronic cholecystitis as seen here, the sinus is associated with some fibrosis and an infiltrate of mononuclear inflammatory cells.
11931.8s gallbladder chronic cholecystitis histopathology Courtesy Barbara Banner MD |
|
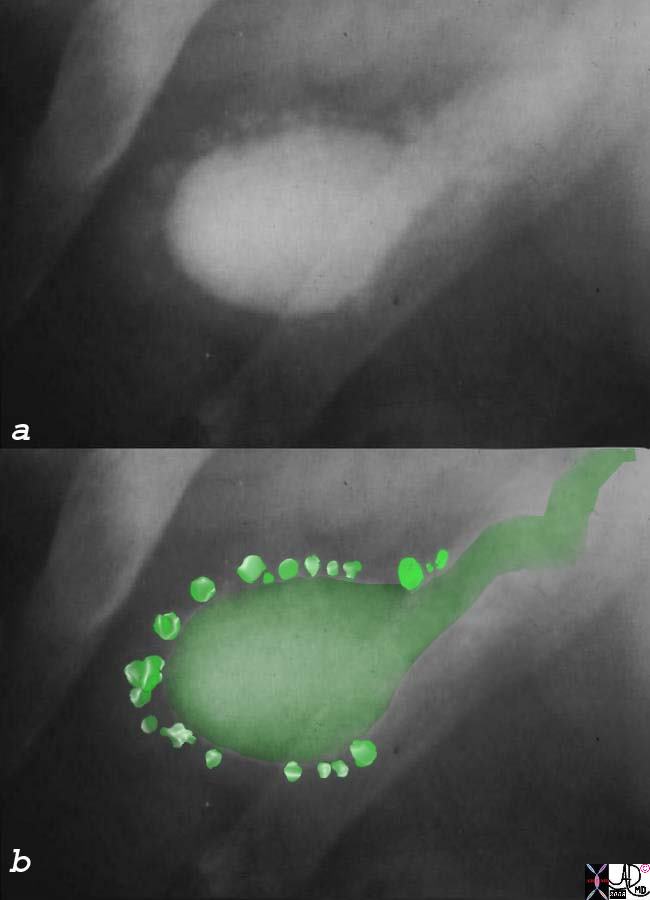
Rokitansky- Aschoff Sinuses |
|
The old fachioned oral cholecystogram best typifies the deep Rokitansky Aschoff sinuses as characterized by deep diverticula which in this cases are scattered around the gallbladder like a pearl necklace. 04743c01s gallbladder contracted outpouchings diverticula prominent Aschoff Rokitansky sinuses hyperplastic cholecystosis hyperplastic cholecystoses adenomyomatosis oral cholycysogram post fatty meal courtesy Ashley Davidoff MD copyright 2008 |
Cystic Arterioles in the Submucosa |
|
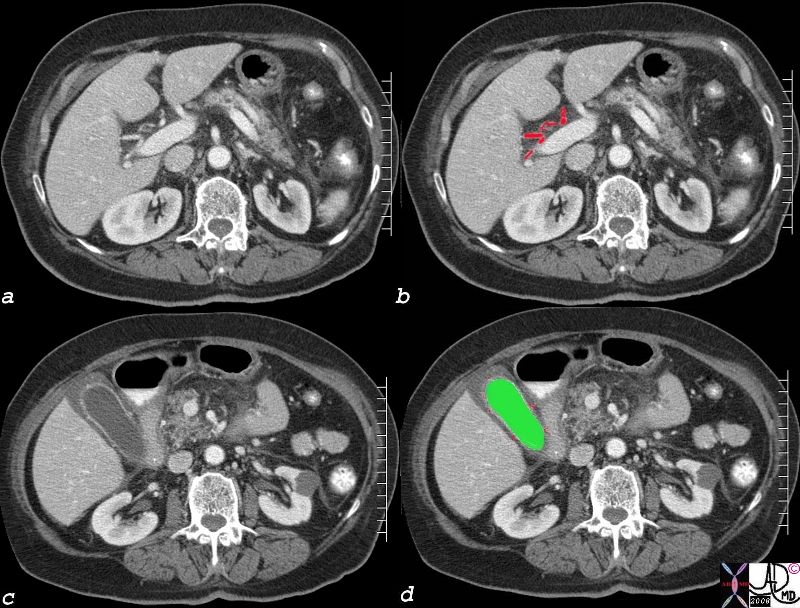
The thickening of the wall noted in the above CT is non specific. It is stated to occur in the “subserosal” layer thus presumably implicating the loose muscular layer but probably also implicating the loose tissue of the serosal/adventitial layers and the lamina propria. The enahancing inner mucosa is seen in c as a white pencil thin line. Below the mucosa and colored in red (image d) the blood vessels in the lamina propria are noted. The edema (gray wall c and d) is noted between the vessels and liver on the right and the vessels and the stomach on the left. Thus the edema probably lies in both the muscularis layer and in the outer serosal/adventitial layer. 82006c04.8s liver gallbladder blood supply hepatic artery cystic artery cystic arterioles wall edema hyperemic mucosa red = hepatic artery green = lumen of the gallbladder CTscan Courtesy Ashley Davidoff MD Copyright 2008 |