
The gallbladder is drained by lymphatics that arise from the lamina propria and serosal adventitial layers and become confluent pass over the anterior and posterior surfaces of the gallbladder, much like the distribution of the arteries. Lymph also drains via lymphatics in the gallbladder fossa directly into the lymphatics of the liver.
From the anterior and posterior wall the main drainage is along the cystic duct to their first nodal station – Calot’s node located within Calot’s triangle near the neck of the gallbladder.
Calot’s Triangle Calot’s Lymph Node Lymphatic Drainage |
| Calot’s triangle is an anatomic space bordered by the common hepatic duct medially, the cystic duct inferiorly and the liver superiorly. The cystic artery usually passes through the triangle, and Calot’s lymph node is also within this triangle. It is an important landmark to recognize during laparoscopic cholecystectomy The first station from the anterior and posterior lymphatic vessels draining the gallbladder is Calot’s node which is seen within the triangle as a pale yellow nodule.
04766b05b04.59ak.8s Calot’s triangle calot’s lymph node anatomy normal Davidoff art copyright 2008 |
From the Calot’s node, there are then two major pathways sometimes via the hepatic nodes. The dominant pathway of lymphatic drainage is the cholecystopancreatic nodes. This pathway courses along the cystic duct and common bile duct and then to nodes that are posterior to the pancreas and the duodenum.

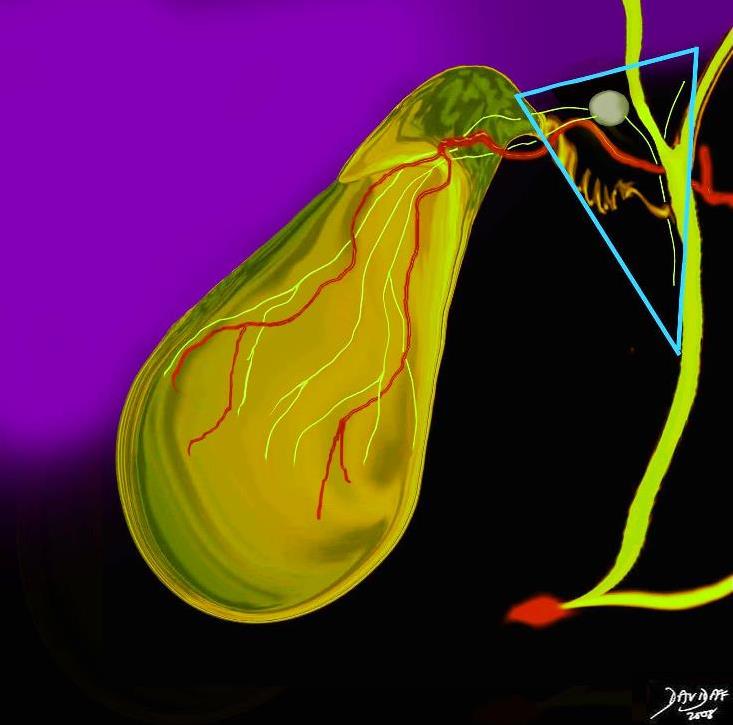
Primary Lymphatic Drainage of the Gallbladder Cholecystopancreatic Pathway |
| The primary pathway of lymphatic drainage of the gallbladder once the lymph reaches the Calot’s node is along the cystic duct, bile duct and toward the nodes that lie behind the head of ht e pancreas and duodenum. In this diaggram one of these nodes is seen as the largest node in close association with the ampulla (red) and pancreatic duct (light pink)
04766b05b04.59dk.8s gallbladder lymphatics Calot’s lymph node blood supply cystic artery anterior branch posterior branch cystic duct common hepatic duct common bile duct Calot’s triangle calot’s lymph node anatomy lymphatic drainage pancreatic node cholecystopancreticoduodenal pathway normal bile duct Davidoff art copyright 2008 Davidoff art copyright 2008 |
The second pathway is the cholecystoceliac where the lymphatics drain from hepatic nodes, and cystic node they pass along the hepatoduodenal ligament close to the foramen of Winslow and drain into to the celiac nodes
The third pathway is the cholemesenteric pathway via the posterior pancreatic nodes and then to aortocaval and paraaortic nodes.
The lymph nodes of the hilum of the liver are usually involved also in the drainage of the gallbladder.
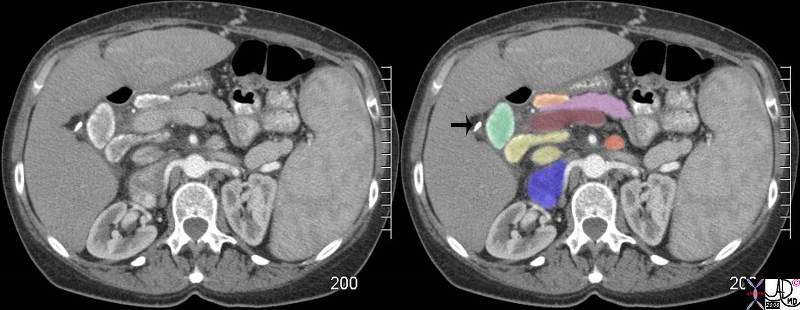 Cystic Lymph Node (green) Among Other Foregut Nodes Cystic Lymph Node (green) Among Other Foregut Nodes |
| 58 year old female with a biopsy proven liver biopsy of sarcoidosis with cirrhosis shows a CT scan through the abdomen with enlarged, lightly calcified nodes where the dominant calcification is on the periphery of the node. These nodes are characteristic of sarcoidosis. The calcified cystic node (green aka Calot’s node) lies medial to the cholecystectomy clip (arrow) The liver is cirrhotic and there is portal hypertension accounting in part for the splenomegaly which may also be enlarged as a result of the sarcoidosis. The portocaval node (yellow) lies between the portal vein (maroon) and the cava (blue). A pancreatic node (light orange) lies anterior and medial to the cystic node and anterior to the neck of the pancreas (pink). A left paraaortic node (orange is the only node on the left side of the foregut group of nodes shown.
82840c02.8s code sarcoidosis lymph node biopsy proven sarcoidosis of the liver with cirrhosis portal hypertension splenomegaly lymph node foregut cystic node node of Calot calcification CTscan Courtesy Ashley DAvidoff MD copyright 2008 |
26477b02arrow |
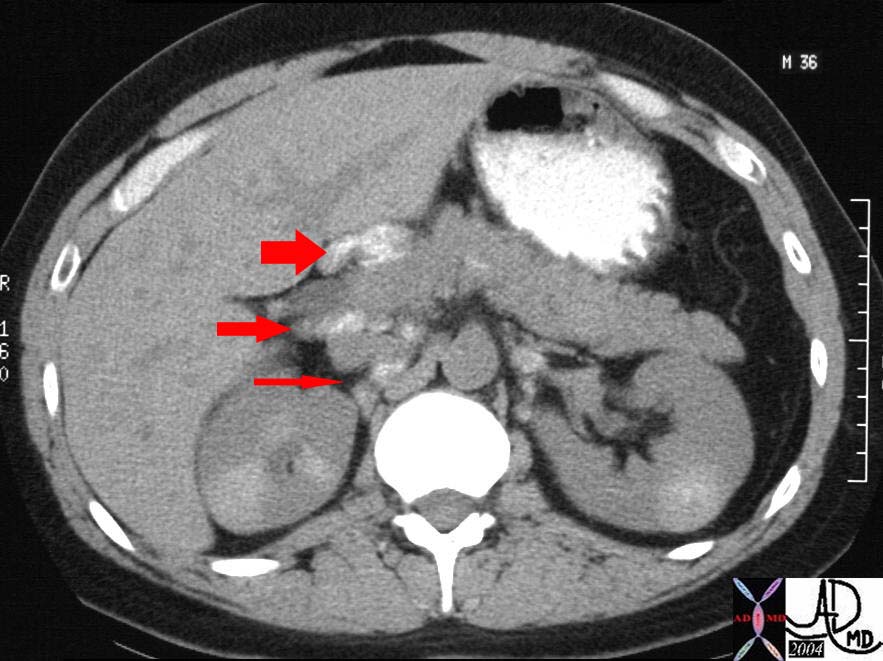
| The CT through the mid abdomen and kidneys is from a patient with sarcoidosis in whom there is extensive but fine calcifications in the kidneys and the celiac axis lymph nodes surrounding the pancreas. These are abnormal lymph nodes but the case serves to demonstrate the lymphatic associations of the head of the pancreas and gallbladder drainage pattern. There are nodes anterior to the head in the porta hepatis (fat arrow), and in the portocaval space posterior to the head. (middle arrow) More posteriorly (thin arrow) small calcified nodes are seen between the IVC and the right crus of the diaphragm.
Courtesy Ashley Davidoff MD pancreas anatomy lymph node lymphatic drainage fx calcified calcification dx sarcoidosis kidney mass calcification calcified imaging radiology CTscan 26477b02arrow |
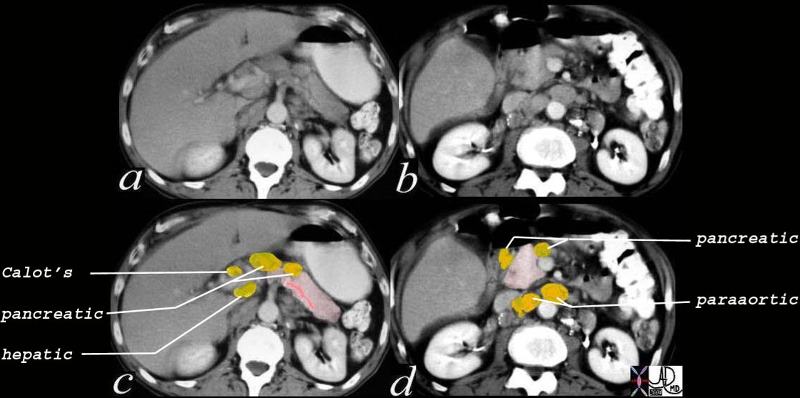
Enlarged Lymph Nodes Relevant to Gallbladder Lymphatic Drainage |
| The CTscan is from a patient with Hodgkin’s lymphoma whose lymph nodes in the abdomen are enlarged. Nodes relevant to gallbladder drainage include Calot’s node, hepatic node, peripancreatic nodes, and paraortic nodes.
40432c02 Courtesy Ashley Davidoff MD code pancreas peripancreatic lymph nodes fx enlarged prominent code dx Hodgkin’s lymphoma imaging radiology CTscan neoplasm malignant tumor |
Histology
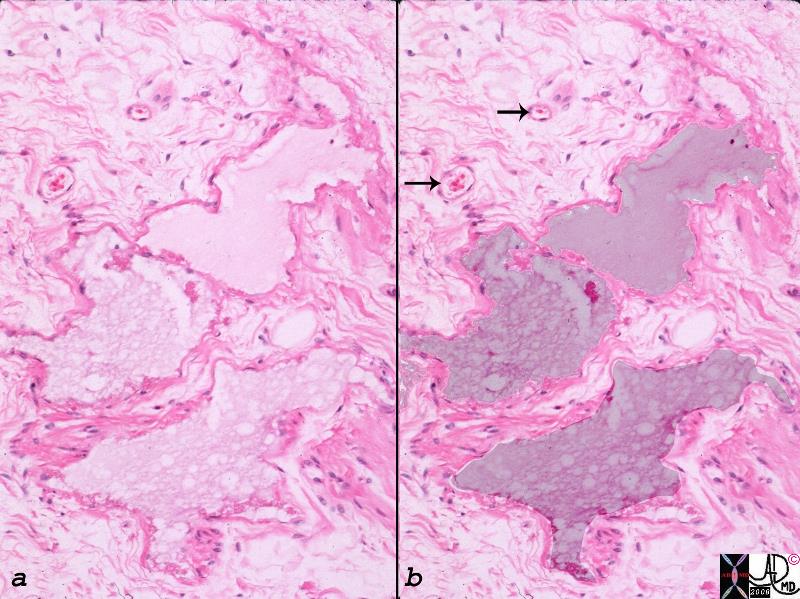
Lymphatic vessels Distended with Lymph |
| The endothelial lined and distended lymphatics (overlaid in dark pink) are identified in the serosal and adventitial layer. The arrows point to associated endothelial lined small blood vessels containing red cells.
00141.1c01.8s Pools of endothelial lined foamy fluid (dark pink) filled vessels represent dilated lymphatics in the gallbladder fossa. Two small endothelial lined capillaries with a few red cells are also seen arrows lymphatics capillaries connective tissue Courtesy Ashley Davidoff MD |
There is a direct route of lymphatic drainage from the gallbladder fossa to the lymphatic channels of the liver through the adventitial surface in the gallbladder fossa.
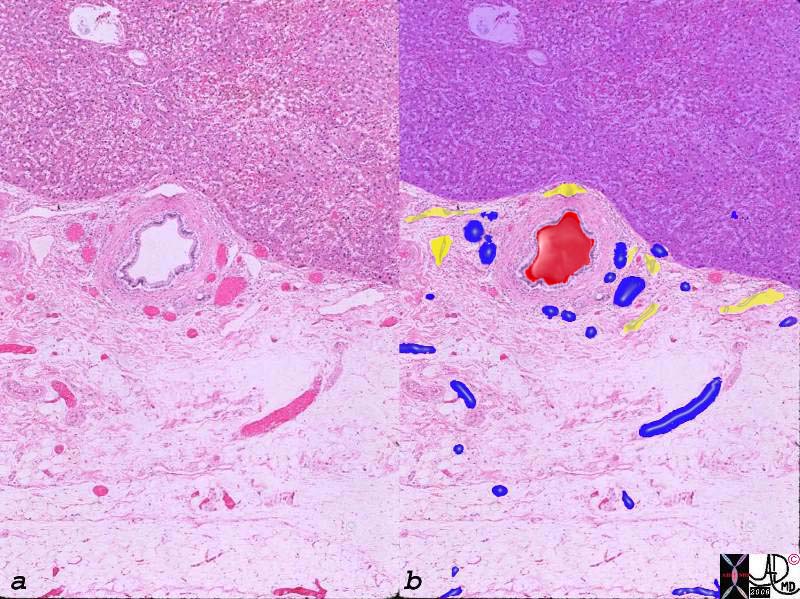
Arteries, Veins and Lymphatics in the Gallbladder Fossa |
|
The histological section of the gallbladder fossa shows the relatively large thick walled branch of the deep cystic artery, abutting the liver (upper portion purple) accompanied by venules (blue) and lymphatics (yellow). The veins and lymphatics drain directly into the liver. 00140c03.8s gallbladder wall gallbladder fossa normal artery duct liver interface histopathology |
Applied Biology
Inflammation of the gallbladder and liver are characterized by exudation of fluid due to hyperemia, and increased capillary leakage as a normal response by the body to the noxious agent. The increased extravascular fluid, may accumulate either by design to dilute the noxious agent or as a result decreased drainage of an overwhelmed lymphatic syatem that fails to drain effectively. As a result fluid may accumulate in the soft tissues of the gallbladder and the fluid is often visible to radiologic imaging.
In acute cholecystitis fluid may accumulate in the wall of the gallbladder, but more specifically pools in the gallbladder fossa .
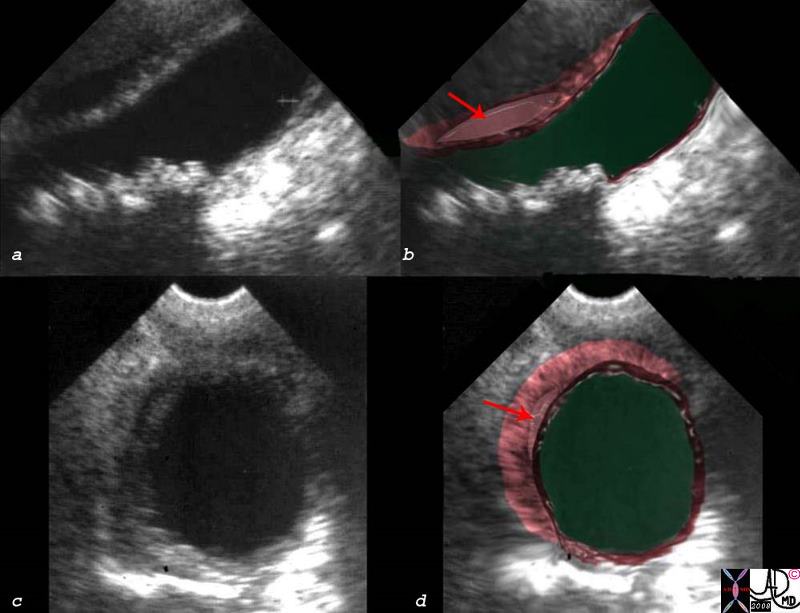
Fluid and Thickening in the Gallbladder Fossa |
| This patient presented with clinical findings that were characteristic of acute cholecystitis. The ultrasound was performed to confirm the clinical suspicion. The ultrasound shows a small amount of fluid (red arrow) in the gallbladder fossa, surrounded by thickened wall.
00543c03s.8 right upper quadrant pain RUQ pain positive Murphy’s sign gallbladder gallbladder fossa thickened linear lacy thickening gall stones calculi calculous multiple small stones stones dependant position shadowing multiple small stones cholelithiasis cholecystitis acute cholecystitis acute calculous cholecystitis USscan ultrasound Courtesy Ashley Davidoff MD copyright 2008 |

Thick Wall Normal Lumen – Hepatitis |
|
The ultrasound above is from a patient with hepatitis. The inflammation of the liver causes increased fluid in the liver and thus slowed venous and lymphatic drainage of the gallbladder. Fluid therefore accumulates in the wall of the gallbladder resulting in thickening. 48008c01 gallbladder thick wall non distended dx hepatitis USscan Davidoff MD |
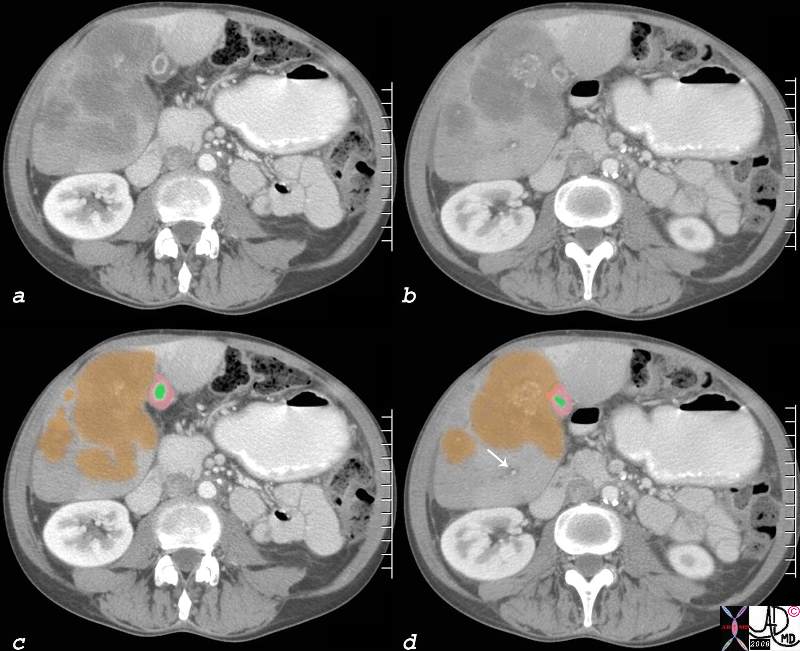
Edematous Galbladder Wall Due to Venous and Lymphatic Congestion |
| 51 year old male with history of rectal carcinoma with extensive hepatic metastases. (orange) The metastases surround gallbladder and by space occupation result in venous and lymphatic congestion causing a thickened edematous gallbladder wall (orange) with a small lumen (green) Tthe portal triad shows surrounding edema (white arrow). This is called periportal tracking which is another sign of venous and lymphatic engorgement. The metastases are calcified confirming the mucinous nature of the tumor.
calcified metastasis in gallbladder fossa edema of the wall lymphatics contracted gallbladder CTscan copyright 2008 Courtesy Ashley Davidoff MD gallbladder liver portal triad 82313c01.8s |
Carcinoma – Lymph Nodes |
|
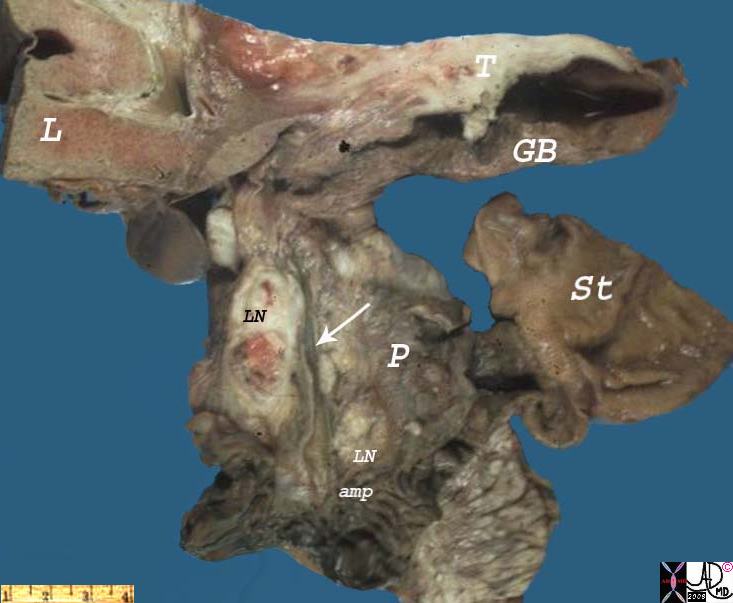
This picture illustrates the major routes of spread of carcinoma (T) of the gallbladder, (GB) which are direct invasion into the liver, (L) and metastasis to regional lymph nodes. (LN) This is a slice taken through the gallbladder and porta hepatis, including small portions of the liver, stomach, and pancreas, from the autopsy of a patient who died of metastatic carcinoma of the gallbladder. The gallbladder wall is thickened by pale tan-white tumor. (T) The same tan-white tumor is present in lymph nodes (LN – black) of the porta hepatis (cystic node) situated along the common bile duct. These lymph nodes can cause extrahepatic biliary obstruction by compressing the common bile duct as they enlarge. The portions of Ampulla of Vater, (amp) stomach (ST) and pancreas seen in this picture are negative for tumor. Not shown is the fact that this tumor invaded directly through the gallbladder wall and directly into the liver. 11949bs gallbadder carcinoma grosspathology Courtesy Barbara Banner MD |