
Copyright 2008
Definition
Oral cholecystography is one of the first studies that used oral contrast in the form of tablets to visualize the gallbladder and the bile ducts. it is mostly of historical interest now, but is still on of the most graphic studies to display adenoyomatosis and the hyperplastic cholecystoses.
Although it has been largely displaced by other imaging modalities. Oral cholecystography offers the ability to evaluate the contents of the gallbladder and detect the presence of stones or obstruction. In many cases, the presence of gallstones, particularly calcium bile can be seen on routine plain films studies. Oral cholecystography is used to enhance these with radioopaque contrast medium that concentrates in the biliary tract after oral ingestion.
Principles
Oral cholecystography can be thought of as plain film x-ray imaging enhanced with contrast medium and utilizes the principles outlined in plain film imaging.
Indications
This study used to be indicated for the evaluation of gallstones within the gallbladder, and to assess the cystic duct for obsturction.
Contraindications
Relative contraindications to this study include impaired hepatic excretion due to liver disease or abdominal illnesses that impair absorption, such as ileus, vomiting or diarrhea as well as contrast allergy.
Advantages
Oral cholecystography is relatively inexpensive and limits exposure to ionizing radiation otherwise associated with computed tomography or scintigraphy.
Disadvantages
There are significant disadvantages associated with oral cholecystography. It requires much longer patient preparation, and thus can not be performed urgently. In addition it may require a second dose of agent if nonopacification of the gallbladder occurs. Sensitivity is low compared to quicker, cheaper, and more comfortable ultrasound.
Aim
The aim of this test is to evaluate for gallstones and the presence of obstruction to the gallbladder.
Method
Patient Preparation
Patients are prepared by taking either tyropanoate sodium or iopanoic acid orally the night before the examination. The drug is absorbed into the bloodstream and excreted from the liver hepatocytes into the bile. Once this is secreted and concentrated in the gallbladder, a plain film x-ray is taken with the patient in any of several views, most often posteroanterior and oblique supine views and an upright or lateral decubitus film are obtained. If non-opacification occurs, a second dose may be obtained or ultrasound performed to confirm obstruction.
Technique
When the patient is examined, it requires the radiologist to examine the patient under fluooroscopy in the supine, oblique, prone and upright postions.
Equipment
Basic fluoroscopic and plain ffilm equipment.
Result
Non-opacification, though not a true positive occurs in 20% of patients. A second dose is given, resulting in opacification in 25% of these cases. Repeated non-opacification is highly reliable with a 95% positive predictive value. False negatives occur approximately 5% of the time.
Examples of Various Diseases
Gallbladder Physiology
 Contracted Post Fatty Meal Contracted Post Fatty Meal |
| This patient was given a fatty meal and the image shows a normally contracting gallbladder
04751 gallbladder contracted gallbladder oral cholecystogram cystic duct normal anatomy oral cholecystogram Davidoff MD |
Gallstones

|
Calcified Stones |
| This is an xray study in which the patient is given a radiopaque substance which is concentrated in the bile in the gallbladder. This study is designed to enhance gallstones. Here the gallstones are partially calcified around their rim and can be seen on their own, as happens about 10% of the time. In addition, the outline of the gallbladder can be seen around the stones because some of the dye got into the gallbladder, indicating that the gallbladder is not obstructed by stones, and that it is still somewhat functional.
gallbladder dx cholelithiasis X-ray Courtesy Barbara Banner MD 11916.8s |

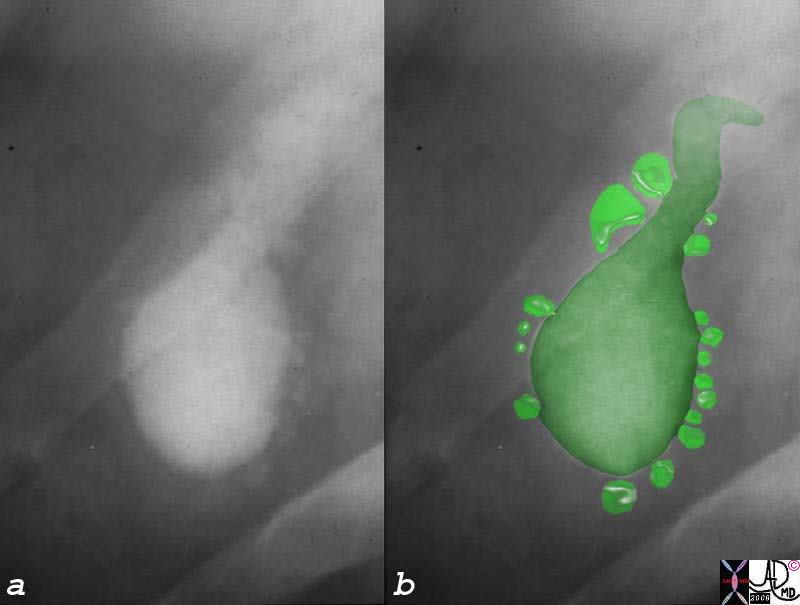
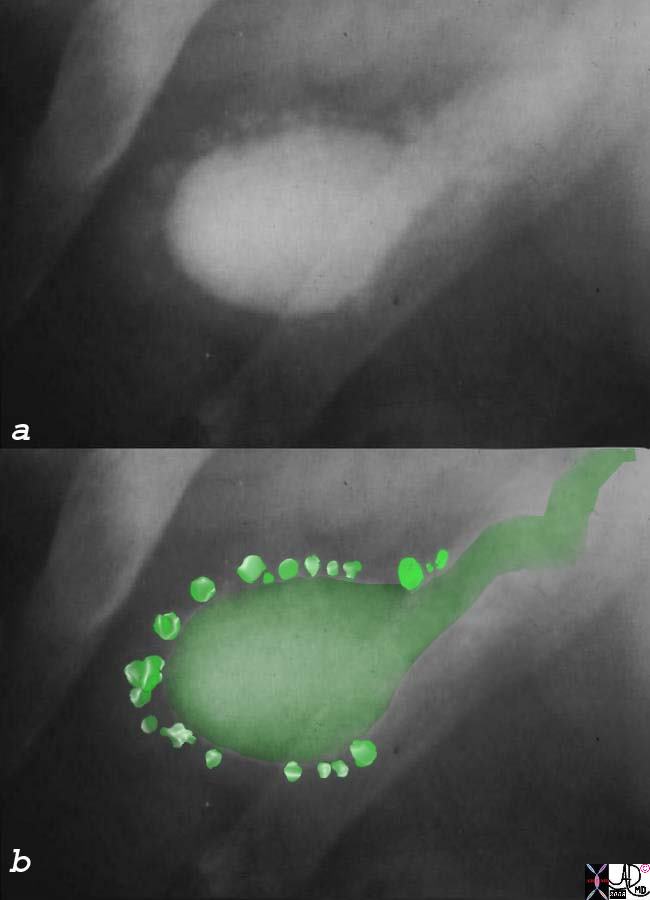
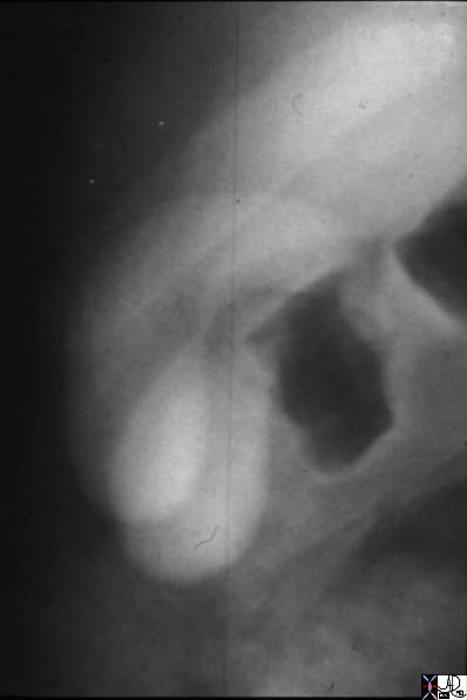
a) Floating Filling defect and Fold in Fundus Oral Cholecystogram – Historical Image 04407 gallbladder filling defect stones cholelithiasis OCG oral cholecystogram imaging radiology historical
b) Stones Floating on Surface – Cholesterol Content – Historical Image |
|
04730 gallbladder floating small filling defect cholesterol stones cholelithiasis OCG oral cholecystogram imaging radiology historical |

Multiple Small Stones Filling the GAllbladder Oral Cholecystogram – Historical Image |
| 04672 gallbladder multiple small stones cholelithiasis OCG oral cholecystogram imaging radiology |
Small Pigmented Stones Lying Dependantly in the Gallbladder |
| 11921.8b05b018.8s gallbladder cystic duct gallstones cholelithiasis Davidoff Art copyright 2008 |
Adenomyomatosis, Hyperplastic Cholecystoses, and Strawberry Gallbladder
|
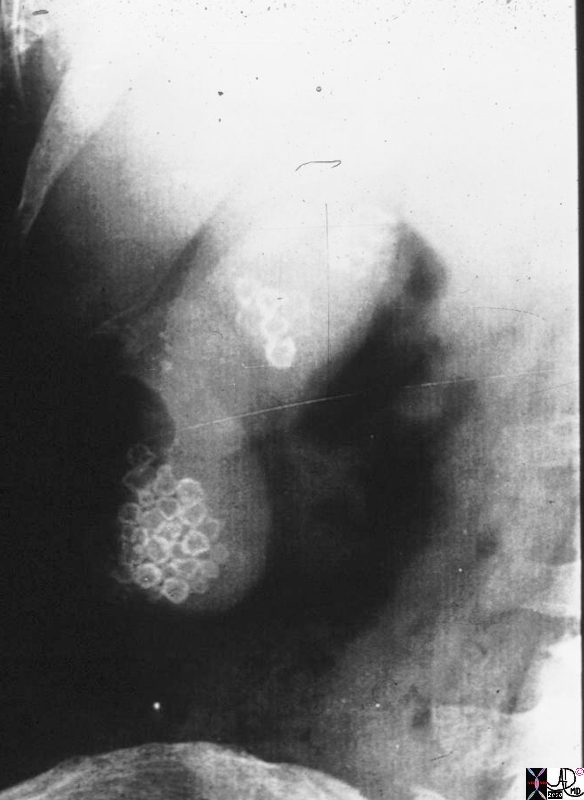
Aschoff-Rokitansky Sinuses |
| 04727c04s gallbladder contracted outpouchings diverticula prominent Aschoff Rokitansky sinuses hyperplastic cholecystosis hyperplastic cholecystoses adenomyomatosis oral cholycysogram post fatty meal courtesy Ashley Davidoff MD copyright 2008 |
|
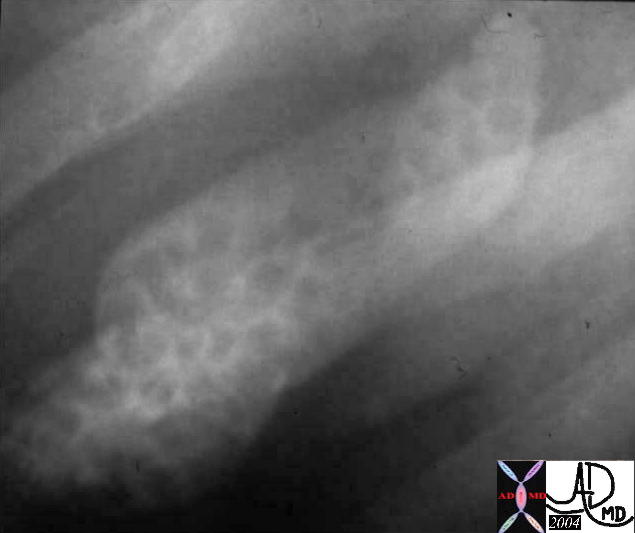
Aschoff-Rokitansky Sinuses |
| 04743c01s gallbladder contracted outpouchings diverticula prominent Aschoff Rokitansky sinuses hyperplastic cholecystosis hyperplastic cholecystoses adenomyomatosis oral cholycysogram post fatty meal courtesy Ashley Davidoff MD copyright 2008 |

Duplication of the Gallbladder
Duplicated Gallbladder |
| 04750 gallbladder duplicated gallbladders oral cholecystogram congenital duplication anomaly growth Davidoff MD |
Conclusion
The study is only of historical interest at this stage
References
Name Doherty, G. M. & Way, L. W. Current Surgical Diagnosis & Treatment Lange Medical Books/McGraw-Hill,