
Copyright 2008
Introduction
The normal gallbladder in the fasting state contains about 50-70mls of bile and measures 8-10 cms in length, by 3-4cms in diameter using ultrasound. Because of its ellipsoid shape the approximation for gallbladder volumecan be estimated by using the formula of length X width X depth X .5cms.
Common Causes
The small gallbladder usually is of lesser clinical significance than the enlarged gallbladder. The most common cause of a small gallbladder is recent ingestion of a meal. In chronic cholecystitis, the development of fibrosis occasionally results in a chronically contracted gallbladder. In HIV cholangiopathies, significant edema of the wall results in impingement on the lumen and the gallbladder will appear relatively small.
Normal Variations
The gallbladder contracts following a fatty meal. Patients are therefore required to fast for 4-6hours before the examination, for optimal evaluation. Examples of contracted gallbladders are shown below.
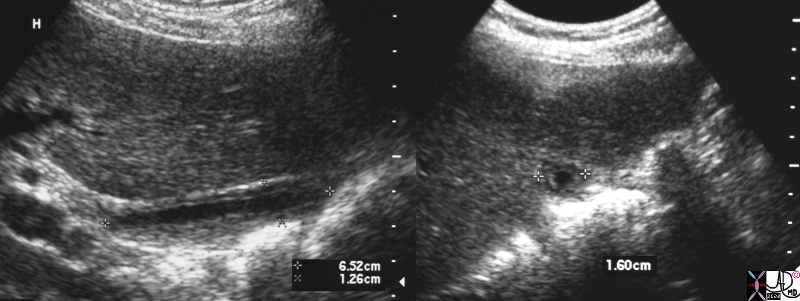
Contracted Gallbladder Following a Fatty Meal |
|
Following a fatty meal, the gallbladder in this instance measures 6.5cms by 1.3cms. 25902c.8s gallbladder small normal post fatty meal normal physiology USscan ultrasound copyright 2008 Courtesy Ashley Davidoff MD |
The fundus has the largest diameter, the body the largest volume while the the neck is the smallest part of the gallbladder proper.

Contracted Gallbladder Recent Meal in Stomach |
|
Image a and b show a transverse CT image revealing a contracted gallbladder with a stomach filled with food (orange). The oral cholecystogram shows a contracted gallbladder following a fatty meal. 46354c01.81s gallbladder function contracted cholecystokinin normal physiology fat digestion size stomach food ingestion stimulated stimulation hormone normal CTscan Courtsy Ashley Davidoff MD radiologists and detectives |

Oral Cholecstogram post Fatty MEal |
|
The oral cholecystogram shows a contracted gallbladder following a fatty meal. 04751 gallbladder contracted gallbladder oral cholecystogram cystic duct normal anatomy oral cholecystogram Davidoff MD |
The Small Gallbladder
The small gallbladder usually is of lesser clinical significance than the enlarged gallbladder. The most common cause of a small gallbladder is recent ingestion of a meal. In chronic cholecystitis, the development of fibrosis results in a chronically contracted gallbladder. In HIV cholangiopathies or hepattis, significant edema of the wall results in impingement on the lumen and the gallbladder which will appear relatively small.
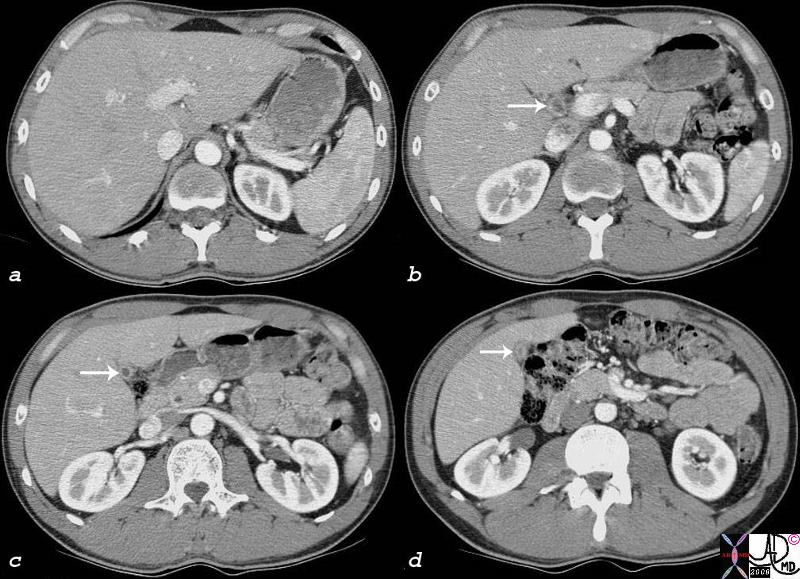
Hypercontractile Gallbladder |
|
The gallbladder in this patient is unusually small. (white arrows b,c,d) There is some fluid and minimal solid content in the stomach that could have been the stimulus. We suspected a hypercontractile gallbladder. 82264c01.8s gallbladder hypercontractile contracted predisposition to adenomyomatosis hyperplastic cholesterolosis small stomach filled with fluid and food particles CTscan Courtesy Ashley Davidoff MD copyright 2008 |

Chronic Cholecystitis, Hyperemic Wall, Small Contracted Gallbladder |
|
The CTscan shows a gallbladder that is small, contains a calcified stone and a hyperemic wall consistent with a fibrotic gallbladder of chronic cholecystitis. these patient are usually not symptomatic. 30701.8s stone cholelithiasis hyperemic wall small contracted chronic cholecytitis stomach gastrostomy redundant mucosa CTscan Courtesy Ashley Davidoff MD copyright 2008 chronic cholecytitis |

Thick Wall Normal Lumen – Hepatitis |
| 48008c01 gallbladder thick wall non distended dx hepatitis USscan Davidoff MD |
Animals Aristotle and Shakespeare
There has been interest in the presence absence and size of the gallbladder in animals. It appears that the presence and size mostly relates to diet so that carnivores tend to have larger gallbladders, omnivores intermediate size and herbivores small or even absent gallbladders. (Hobart) The Petromyzon is a sea lamprey that is an eel like jawless fish that parasitises on healthy fish by attaching to them. They are born with a biliary system which subsequently degenerates. In the pigeon the gallbladder also develops and then disappears. In the rat horse, zebra, camels, rhinos, elephants, dolphins, and deer the gallbladder never develops(Mann) (Robinson) Aristotle discussed this in his treatise on animal anatomy in 350BC.
Shakespeare seemed to have been familiar with the absence of gallbladders in pigeons “But I am pigeon-liver’d and lack gall ” Hamlet: II, ii
Applied Biology
The size of the gallbladder is one of the more important determinants in the evaluation of gallbladder disease, but as you will learn there is not always a black and white answer as to whether the gallbladder is enlarged or not.
The size of the gallbladder cannot be assessed by clinical examination since the gallbladder lies under the liver and only a small portion of the fundus is exposed. Therefore under normal circumstances it cannot be palpated and is only palpable when it is significantly enlarged. For this reason, assessment of the size of the gallbladder requires the use of an imaging technique. This is best accomplished by ultrasound, since the true long axis and short axis can be defined by the ultrasonographer who is able to angle the transducer along the appropriate axis. The gallbladder is normally positioned at an angle that is off the horizontal, sagittal and coronal planes. The fundus is located relatively inferiorly, while the neck is positioned more medially and superiorly. Thus by the nature of the transverse imaging of CT and usual orthogonal imaging of MRI, the true axis is not routinely defined by these methods. Although nuclear imaging can also assess the size of the gallbladder accurately, other factors such as wall thickness and probe tenderness cannot be evaluated. Thus when assessment of the size of the gallbladder, and associated features of wall thickness and probe tenderness is required, ultrasound becomes the procedure of choice.
From a practical and clinical standpoint, the clinician who suspects an enlarged gallbladder is really asking whether there is increased pressure in the gallbladder. The imaging technology uses size as an indirect measure of the intraluminal pressure since we would otherwise have to use invasive techniques to assesss the pressure directly. Since there are situations where the gallbladder loses its tone (atonic or hypotonic gallbladder as a result of aging process or diabetes) it can enlarge without the ever important increase in pressure. On the other hand there are situations when the gallbladder wall is fibrotic (chronic cholecystitis) and this results in a small contracted gallbladder which cannot dilate when the luminal pressure rises.
Multiple factors therefore have to be taken into consideration when assessing the size of the gallbladder.
The key to assessing gallbladder size is a transverse view through the body. This requires a transverse image that is orthogonal to the long axis of the gallbladder. In this view as shown below the transverse (right side to left side) dimension is larger than the anteroposterior (A-P) dimension. This is normal. It implies that that the luminal pressure is less than the pressure exerted by the liver and so the liver flattens the anterior wall. Sometimes the normal gallbladder has a larger A-P dimension depending on the external forces exerted on it. It is not usually round. The normal largest dimension in the transverse should not be greater than 4-5cms.
The normal gallbladder in the fasting state contains about 50-70mls of bile and measures 8-10 cms in length, by 3-4cms in diameter using ultrasound. The volume is determined by using the formula of ellipsoid approximation, – length X width X depth X .5cms.
The size of the gallbladder is one of the more important determinants in the evaluation of gallbladder disease, but as you will learn there is not a black and white answer as to whether the gallbladder is enlarged or not.
The size of the gallbladder cannot be assessed by clinical examination since the gallbladder lies under the liver and only a small portion of the fundus is exposed. Therefore under normal circumstances it cannot be palpated and is only palpable when it is significantly enlarged. For this reason, assessment of the size of the gallbladder requires the use of an imaging technique. This is best accomplished by ultrasound, since the true long axis and short axis can be defined by the ultrasonographer who is able to angle the transducer along the appropriate axis. The gallbladder is normally positioned at an angle that is off the horizontal, sagittal and coronal planes. The fundus is located relatively inferiorly, while the neck is positioned more medially and superiorly. Thus by the nature of the transverse imaging of CT and usual orthogonal imaging of MRI, the true axis is not routinely defined by these methods. Although nuclear imaging can also assess the size of the gallbladder accurately, other factors such as wall thickness and probe tenderness cannot be evaluated. Thus when assessment of the size of the gallbladder, and associated features of wall thickness and probe tenderness is required, ultrasound becomes the procedure of choice.
References
Dodds, Wylie
Pathology Outlines: Gallbladder